Download as KEY, PPTX

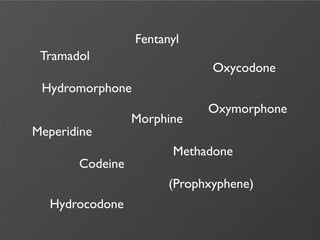
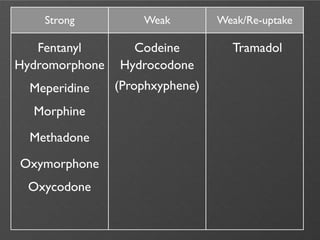
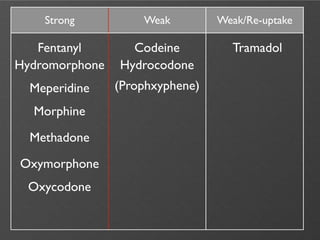
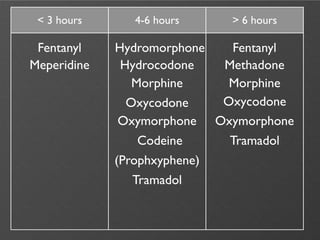
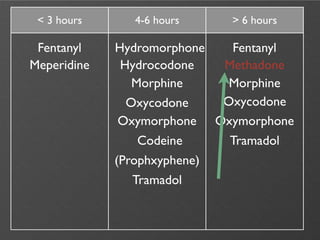


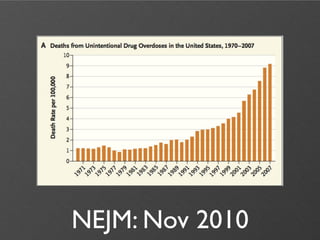
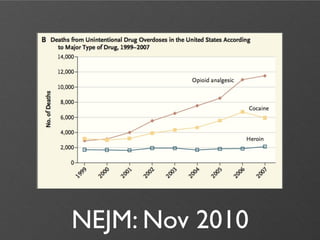
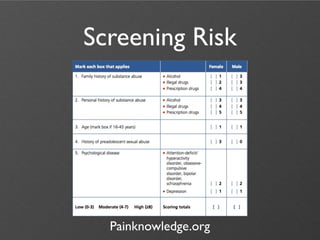
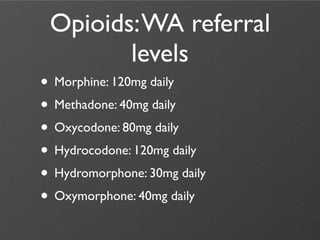
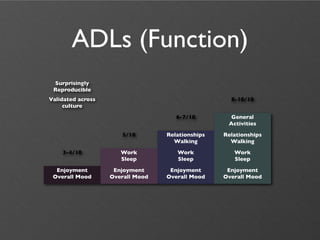





The document discusses the use of opiates in managing chronic non-malignant pain, highlighting different types of opioids, their dosing, and the associated risks of abuse and overdose. It examines physician prescribing variations and emphasizes the importance of assessing analgesia, function, and possible adverse reactions. Additionally, it touches on guidelines for safe opioid prescribing and considerations for managing aberrant behaviors in patients.














































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


