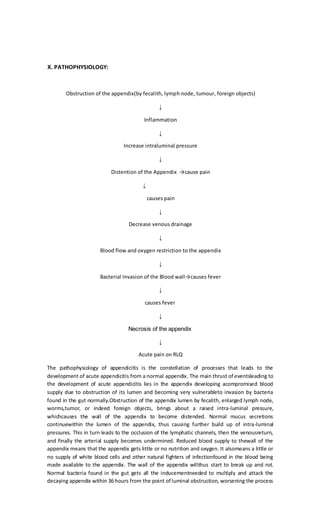
T.A., an 18-year-old male, presented to the emergency room with severe right lower quadrant pain and was diagnosed with acute appendicitis. He underwent an emergency appendectomy a few hours later. Appendicitis is caused by obstruction of the appendix, usually by infection or fecal matter, leading to inflammation, distention, and restricted blood flow. Without timely removal of the infected appendix, complications like perforation and infection of the abdominal cavity can occur. The patient's postoperative recovery was unremarkable.