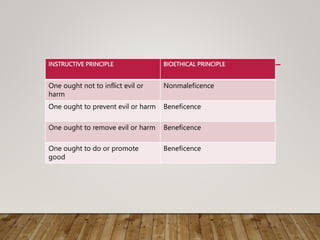
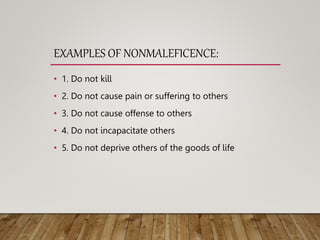
This document discusses the principle of nonmaleficence in medical ethics. It defines nonmaleficence as the obligation to not inflict harm, based on the maxim "first, do no harm" from the Hippocratic tradition. The principle helps guide decision-making around issues like killing, treatment withdrawal, and use of ordinary vs extraordinary measures. It distinguishes nonmaleficence from beneficence, provides examples of nonmaleficence, and discusses practical applications like withholding/withdrawing treatment and ordinary/extraordinary measures.