INTRODUCTION
One of themain objectives of modern
anesthesia is to ensure adequate depth
of anesthesia.
To prevent awareness in patients without
overloading them with potent drugs.
Various methods have been described
from time to time to measure the depth
of anesthesia.
DEFINITION
Intraoperative awarenesswith recall refers to intraoperative
consciousness and postoperative explicit recall of operative events
While it is a rare complication, it can potentially be devastating.
9.
RECALL
• It isthe patient’s ability to retrieve stored memories
• Assessed by a patient’s report of previous events, in particular,
events that occurred during general anaesthesia.
Recall can be either explicit or implicit.
• Explicit memory: It refers to intentional or conscious
recollection of prior experiences as assessed so called direct
memory test.
• Implicit memory (perception without conscious recall): The
patient denies recall, but may remember “something” under
hypnosis.
10.
Implications
of
Awareness
There areapproximately 1 to 2 cases of
intraoperative awareness per 1000
administrations of general anaesthetic, and
among those with intraoperative awareness
with recall, 43% develop post traumatic stress
disorder.
11.
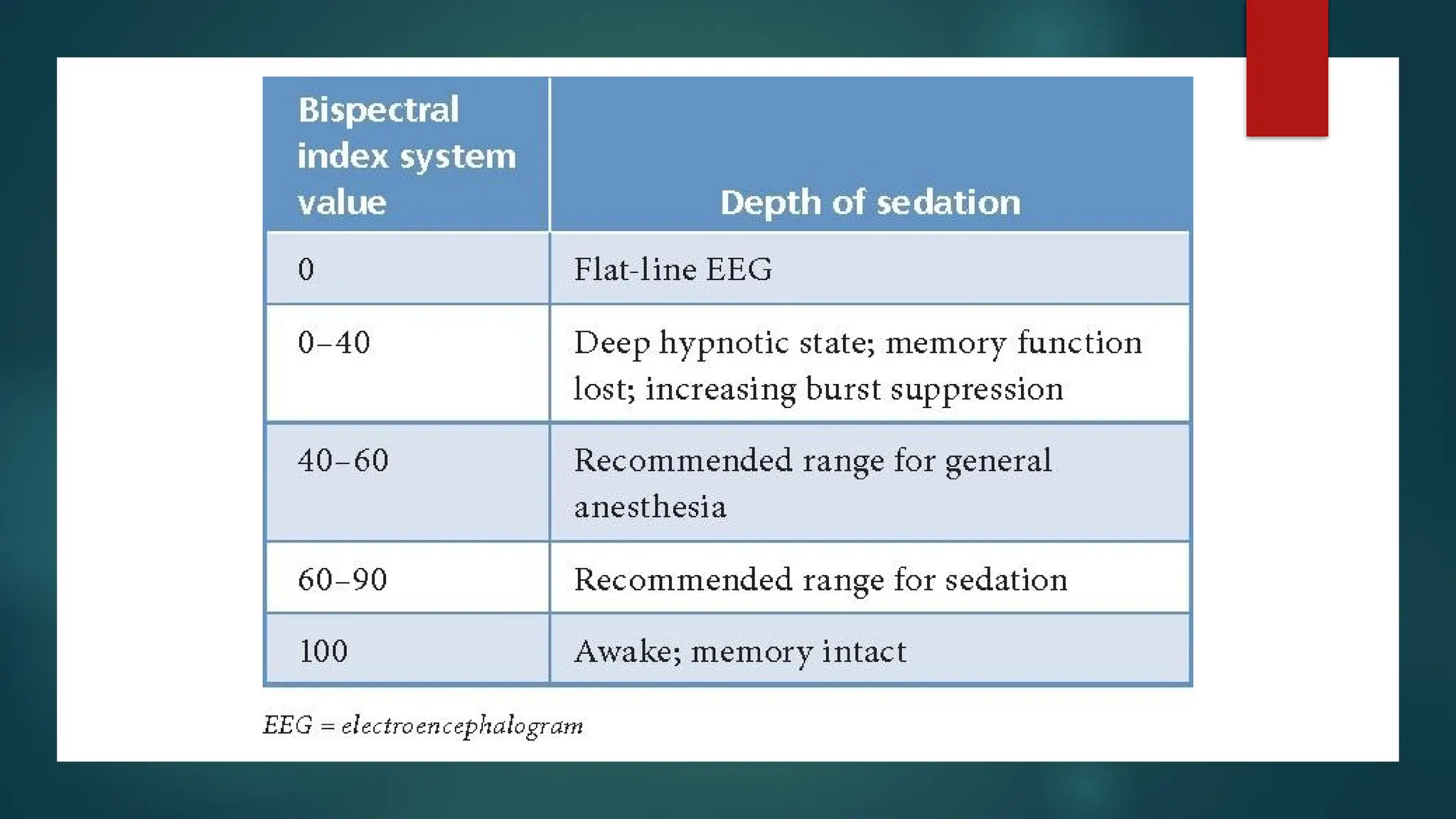
BISPECTRAL INDEX MONITORING
Bispectral monitoring is a monitoring method used in ICU and OT to
directly measure the effects of sedatives on brain by recording
electrical activity via Electroencephalogram(EEG).
12.
Why do we
needBIS
Reduces the risk of intraoperative
awareness
Improves patient safety
Helps tailor anesthetic doses
Helps minimize drug withdrawal
symptoms
13.
Advantages
of BIS
monitoring
Reduced riskof adverse events- intraoperative
awareness, nausea, vomiting, and delirium.
Faster recovery- help patients emerge from
anesthesia faster and shorten their stay in the
recovery room.
Reduced anesthetic- help clinicians better titrate
their medications, which can reduce the amount of
anesthetic used.
Improved patient satisfaction- by reducing
postoperative nausea and inadequate hypnosis.
Better orientation- help patients regain
orientation in time and place after surgery.
14.
Uses
High-risk patients
Pediatric surgeries:Tonsillectomies and adenoidectomies in children
aged 3 to 18 years
Cardiac surgery: To maintain a stable depth of anesthesia and reduce
the risk of awareness and hemodynamic instability
Neurosurgery: To maintain an appropriate level of sedation while
allowing for neurological evaluations
Obstetric surgery: To balance the depth of anesthesia and ensure
maternal comfort while minimizing fetal exposure to anesthetic agents
Emergency and trauma surgery: To provide real-time data for rapid
adjustments to anesthesia levels
15.
EQUIPMENT
BIS sensor
BISx (digital signal converter and processing
unit) with the monitor interface cable and the
patient interface cable (PIC)
BIS monitor.
16.
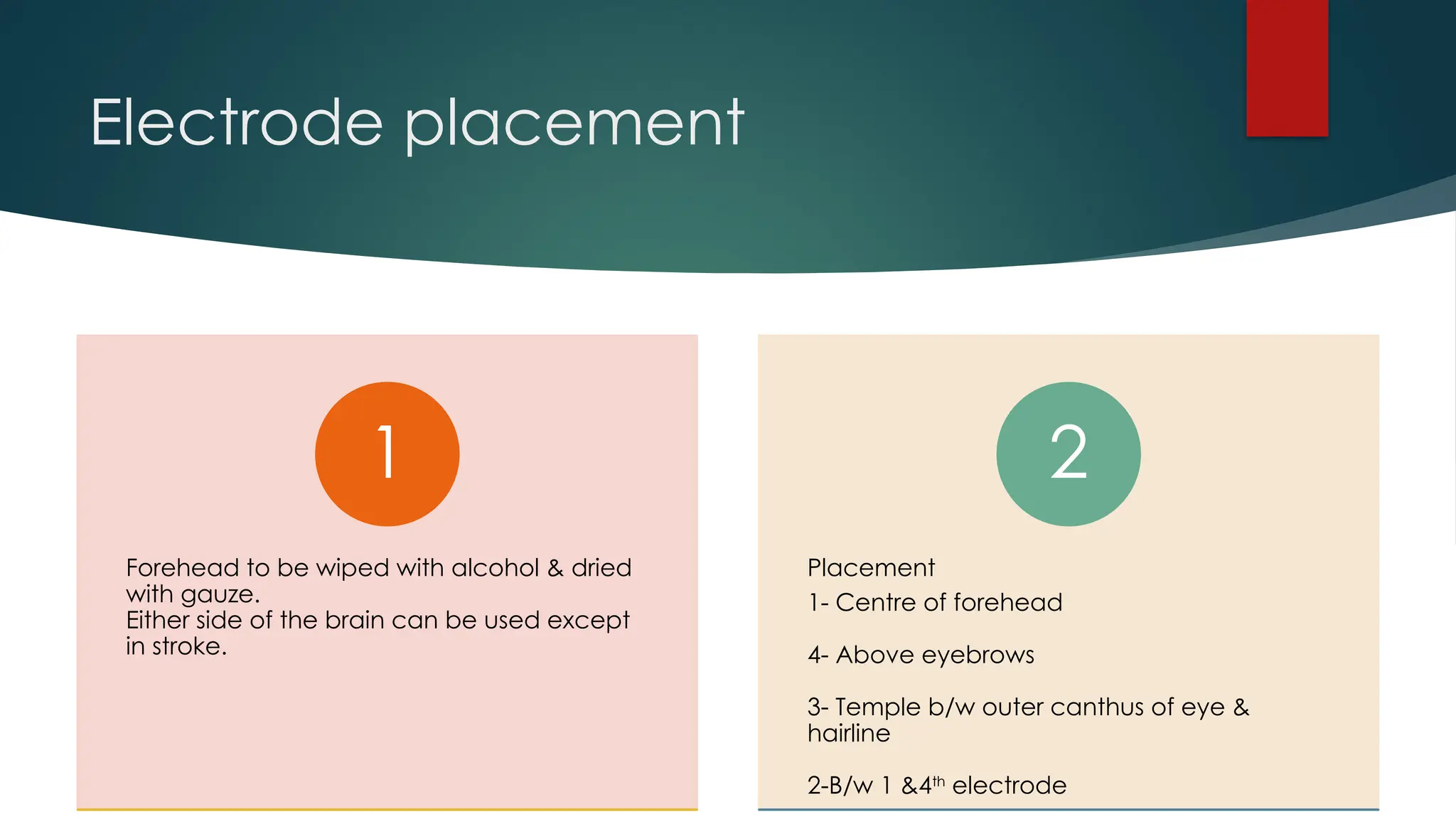
Electrode placement
Forehead tobe wiped with alcohol & dried
with gauze.
Either side of the brain can be used except
in stroke.
1
Placement
1- Centre of forehead
4- Above eyebrows
3- Temple b/w outer canthus of eye &
hairline
2-B/w 1 &4th
electrode
2
18.
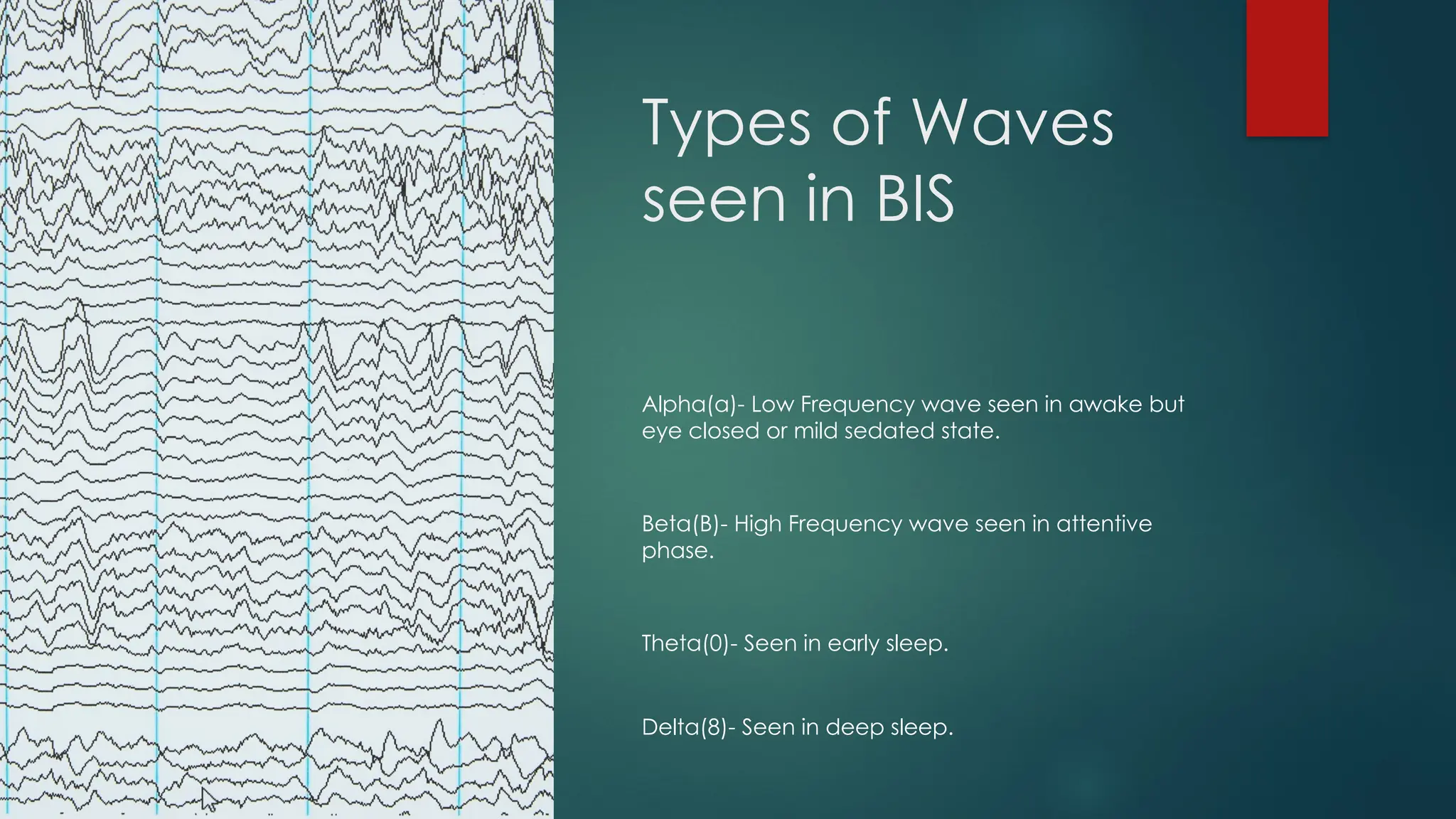
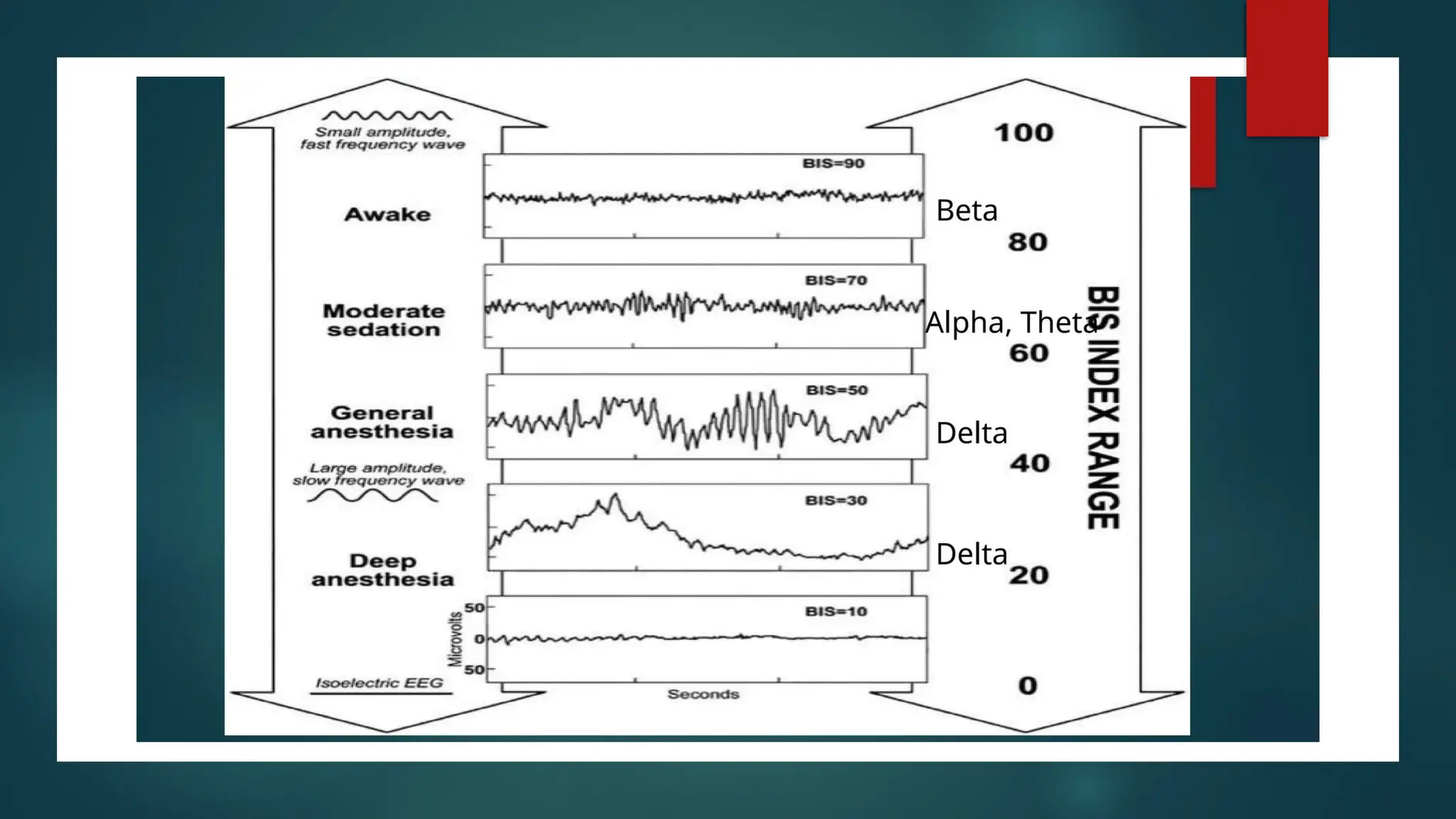
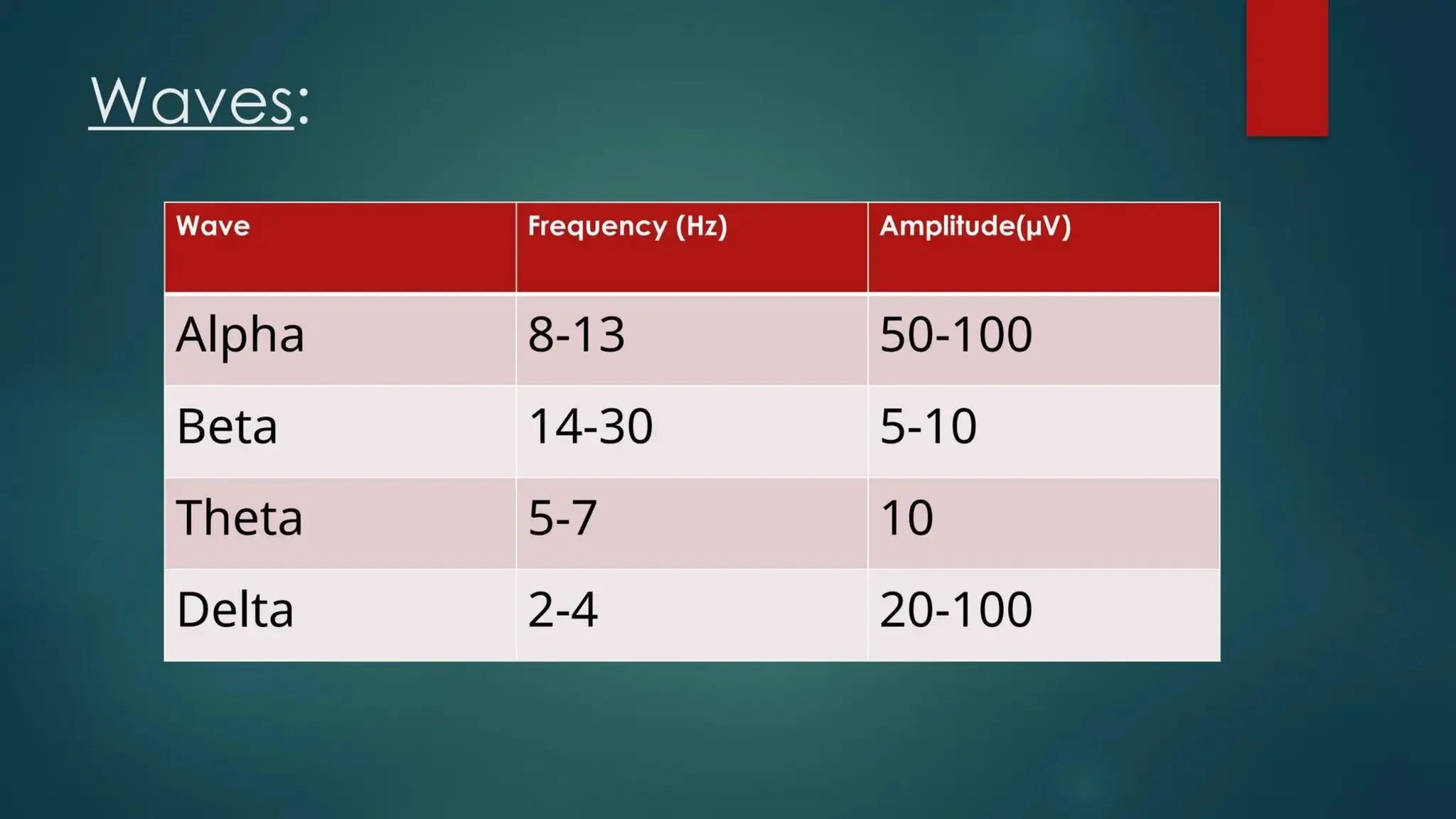
Types of Waves
seenin BIS
Alpha(a)- Low Frequency wave seen in awake but
eye closed or mild sedated state.
Beta(B)- High Frequency wave seen in attentive
phase.
Theta(0)- Seen in early sleep.
Delta(8)- Seen in deep sleep.
22.
INTERFERENCE
Artifacts
Medications
Muscle tone
Anesthetic
Patient characteristics-Femalepatients, patients with a
lower BMI, and elderly patients may have different BIS
values
Position
Electrical devices-Pacemakers and cautery can
introduce high-frequency signal artifacts and lead to high
BIS values
Neurological disorders
Psychoactive medications
Age
Cerebral Hypoxia
Cerebralhypoxia refers to a condition in which there is a decrease of
oxygen supply to the brain even though there is adequate blood flow.
Complications of general anesthesia can create conditions that can lead to
cerebral hypoxia.
Symptoms of mild cerebral hypoxia include inattentiveness, poor judgment,
memory loss, and a decrease in motor coordination.
Brain cells are extremely sensitive to oxygen deprivation and can begin to
die within five minutes after oxygen supply has been cut off.
When hypoxia lasts for longer periods of time, it can cause coma, seizures,
and even brain death.
25.
INTRODUCTION
Cerebral oximetersare non-invasive, continuous monitoring devices,
used to monitor adequate cerebral oxygenation.
They utilize similar physical principles to pulse oximeters
Use NIRS to obtain continuous non-invasive measurements of
cerebral oxygenation values
26.
History
The first commerciallyavailable
cerebral oximeters were used in
the 1990s
However, Jobsis first introduced
the concept of using near-infrared
spectroscopy (NIRS) to measure
cerebral oxygenation in 1977.
27.
COMPONENTS
1. Light source
Emitslight in the near-infrared (NIR) spectrum,
typically between 700 and 870 nanometers
The light can be emitted using light emitting
diodes(LED) or by stimulated emission of
radiation
2. Light sensors
Detect the scattered and unabsorbed light
that returns to the surface
Embedded in the adhesive pads of the
oximeter probe
3. Monitor
Calculates cerebral oxygenation using the
Beer–Lambert law
Displays the results as regional hemoglobin
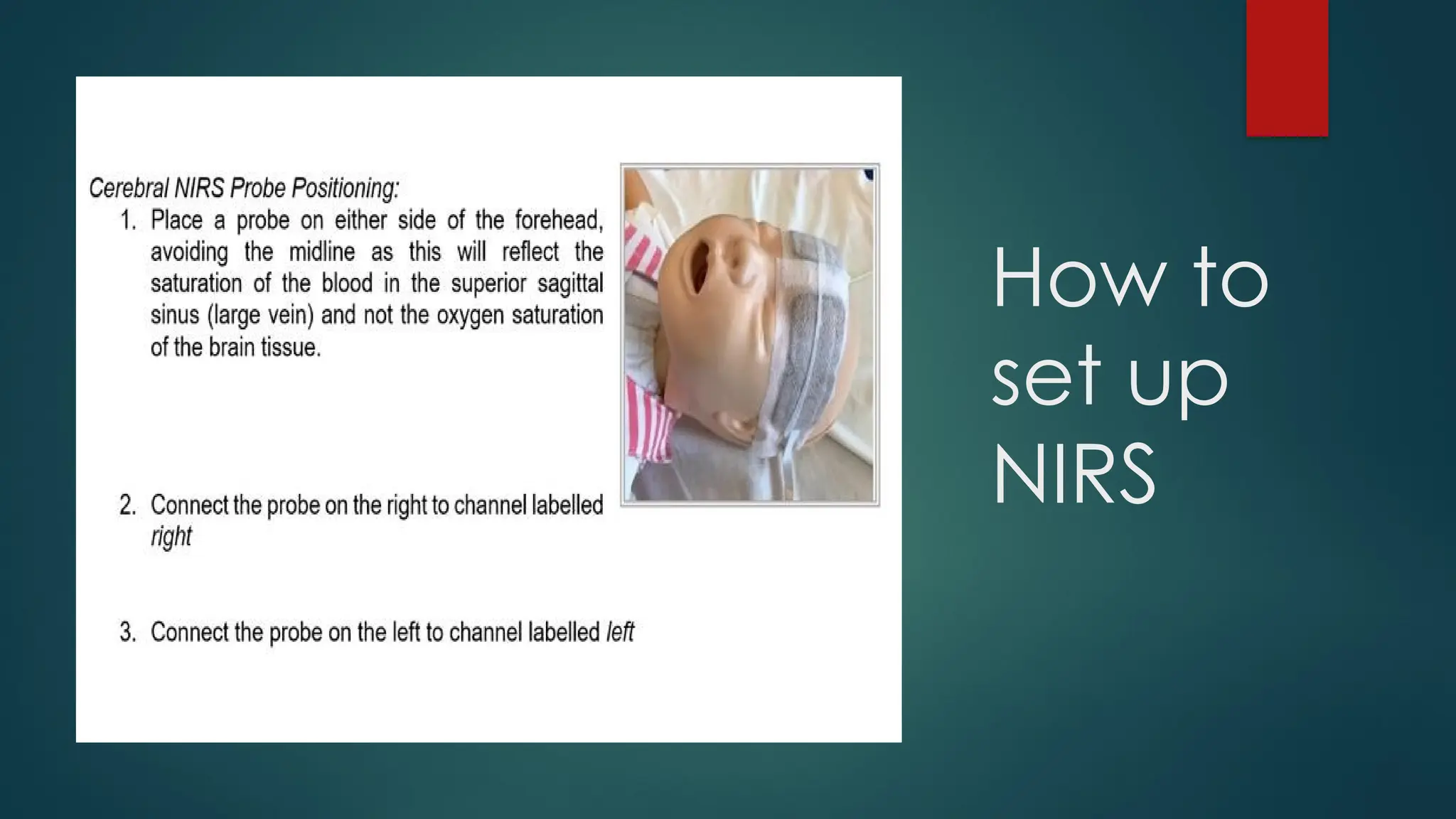
28.
COMPONENTS
4. Probe
Contains thelight source and light sensors
Attached to the patient’s scalp using adhesive
pads
Most commonly placed on the forehead
5. Tissue
The light penetrates the skull and brain, and is
absorbed by chromophores like hemoglobin,
bilirubin, and cytochrome
The amount of light absorbed depends on the
oxygenation status of the hemoglobin
29.
Uses
Cardiac surgery: Cerebraloximetry can help identify
patients at risk, detect malpositioned cannulae, and
monitor oxygenation during cardiopulmonary bypass
Traumatic brain injuries: Cerebral oximetry can help
diagnose cerebral ischemia and hypoxia, and
identify intracranial hematomas
Neonatal care: Cerebral oximetry is widely used in
neonatal care
Neurology: Cerebral oximetry is used in neurology to
monitor brain oxygenation
Anaesthesia: Cerebral oximetry is used in general,
cardiac, thoracic, vascular, and
neuroanaesthesia
30.
Physics
Light sources releaselight in the infrared range
through a process of either stimulated emission of
radiation or through light-emitting diodes.
Emitted light in the infrared range is able to penetrate
the skull to reach underlying cerebral tissue.
Emitted light is either absorbed, redirected, scattered,
or reflected.
When infrared light contacts haemoglobin, a change
in the light spectrum occurs, depending upon the
oxygenation status of the haemoglobin molecule.
Reflected light returns towards the surface and is
detected by the light detectors within the oximetry
probes.8
31.
Beer Lamberts
Law
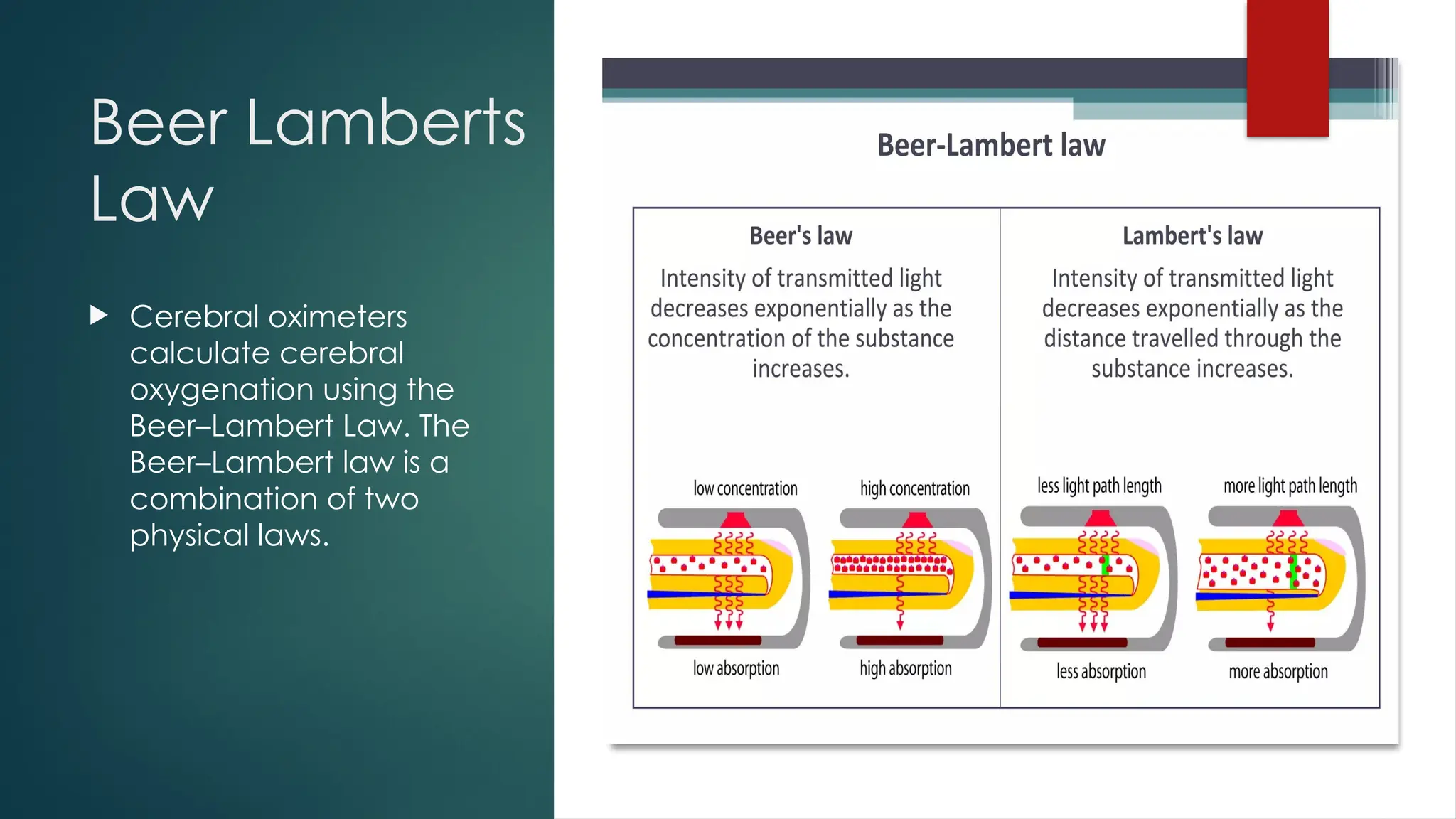
Cerebraloximeters
calculate cerebral
oxygenation using the
Beer–Lambert Law. The
Beer–Lambert law is a
combination of two
physical laws.
32.
Clinical
interpretation
Baseline cerebral oximetryvalues should be obtained before
induction of anaesthesia.
Normal values range from 60% to 80%
Anatomical variations, e.g. incomplete Circle of Willis, severe
carotid artery stenosis can create errors in cerebral oximetry values
therefore, it is recommended that cerebral oximetry is performed
bilaterally
Cerebral oximetry values must not be interpreted in isolation
Alterations in cerebral oximetry measurements must take into
consideration all available clinical information and physiological
state of the patient.
Further Considerations
Skincare
Skin integrity should be routinely monitored by gently peeling back the fixing to reveal
the area under the probe every 6 hours.
The probe must have good contact with the skin and secured with proper fixing.
Avoid the use of any moisturising lotions on the skin and ensure the probe is closely
adhered to skin.
Renewing Probe
Probes are single patient use and should only be renewed if they stop working or has
become visibly damaged.
Discontinuation of NIRS Monitoring
Should only be done following discussion with the Consultant Intensivist and ought to
be considered if the patient is extubated successfully and demonstrates
haemodynamic stability
36.
Limitations
Blood from anextracranial source can create
erroneously low measurement.
Electrosurgical equipment, that is, diathermy,
can affect the accuracy of measurement.
Cerebral oximeters only measure regional
cerebral oxygenation. Large areas of the
brain remain unmonitored.
Cerebral oximeters are unable to identify a
cause for the desaturation.
37.
Entropy
Entropy monitoris an EEG-based monitor that is used in combination
with standard clinical monitoring and clinical skills to indicate the
patient’s response to anesthetic drugs during surgery
38.
Indications
Entropy isindicated for adult and pediatric
patients aged 2 years and older within a
hospital for monitoring the state of the brain.
The measurement can be started, and
stopped, at any time during the operation.
39.
Contraindications
Pediatric patients youngerthan the age of 2 years
Those undergoing procedural or conscious sedation
Seizure activity may also cause interference
Patients with neurological disorders, traumas, or their sequelae
When using benzodiazepines, nitrous oxide, or ketamine as sole
anesthetic agents.
Psychoactive medication or very high opiate doses may slow down
the EEG activity; hence, decreasing its entropy values
40.
Components
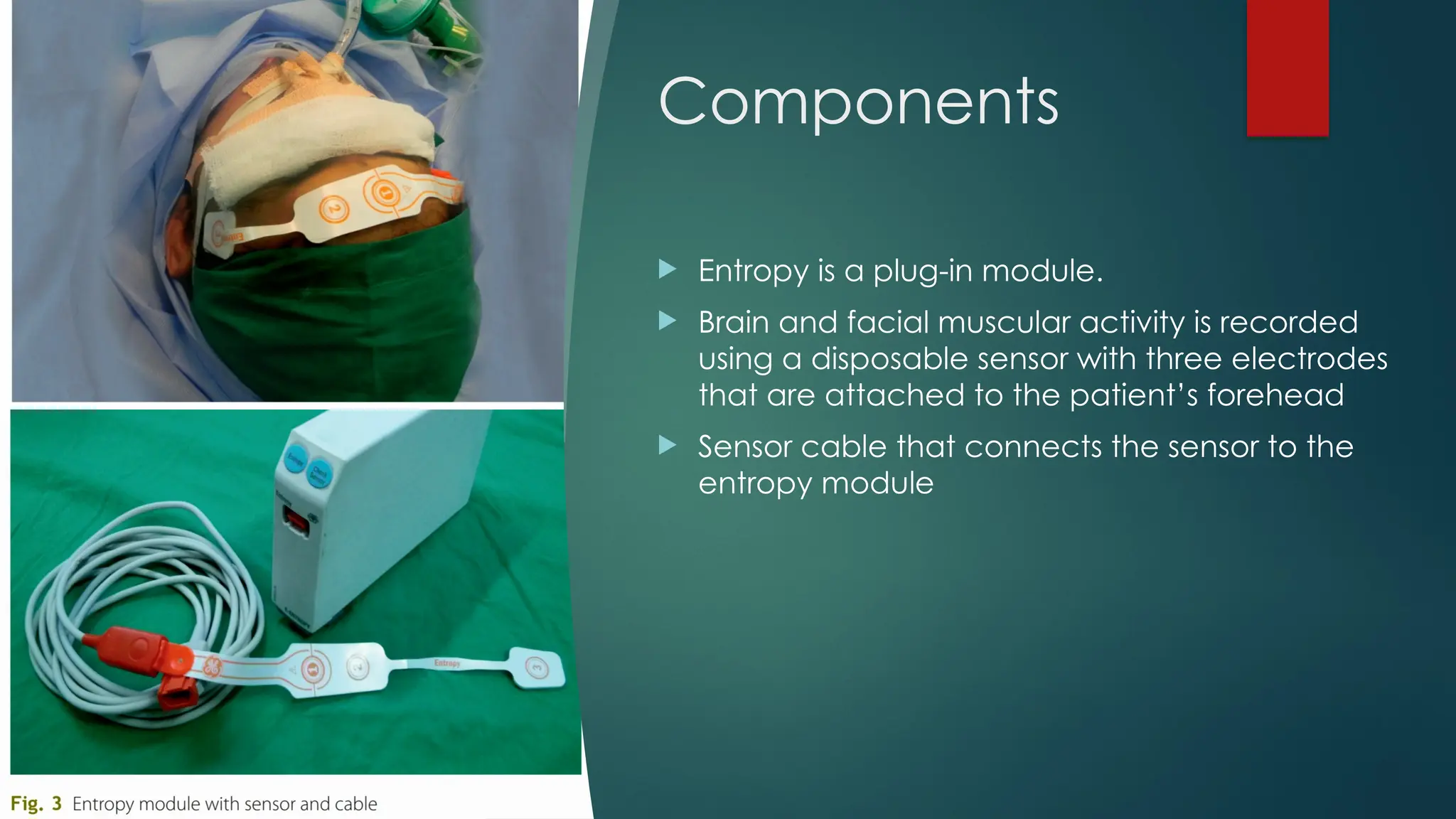
Entropy isa plug-in module.
Brain and facial muscular activity is recorded
using a disposable sensor with three electrodes
that are attached to the patient’s forehead
Sensor cable that connects the sensor to the
entropy module
41.
How it works
The entropy monitor measures irregularity in spontaneous brain and
facial muscular activity, using a proprietary algorithm to process
EEG and frontal electromyography (EMG) data
After that, the signal is divided into two frequency bands (0.8–32 Hz
and 0.8–47 Hz) of
spectral entropy or state entropy (SE)- 0.8–32 Hz
response entropy (RE)-0.8–47 Hz
The monitor performs the burst suppression (BS) analysis and displays
the burst suppression ratio (BSR).
43.
Interpretation
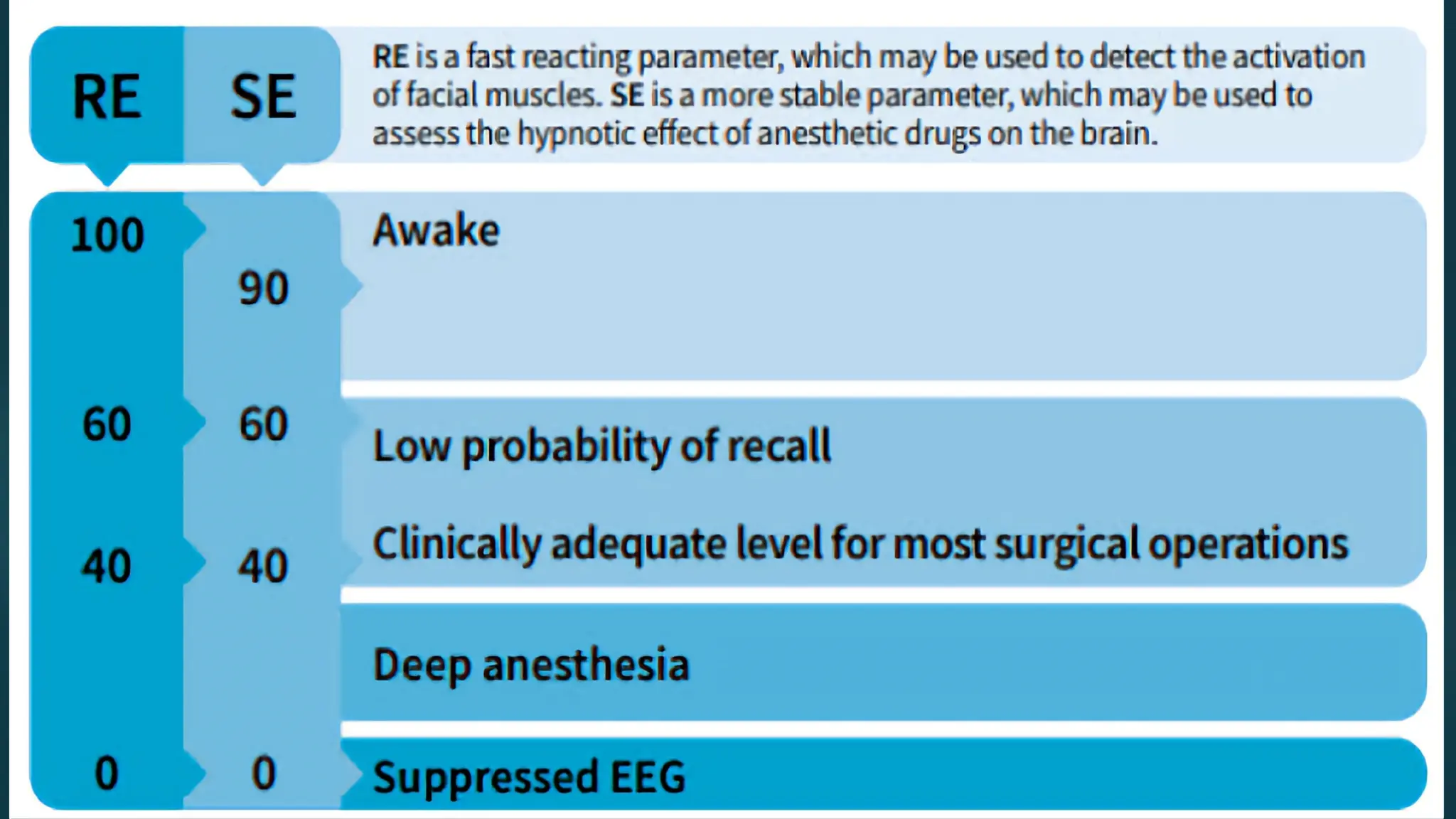
The target rangefor entropy value is 40–60.
RE and SE values near 40 indicate a low probability of
awareness with recall.
SE includes information only from EEG, the RE also includes the
EMG activity
When the RE and SE values are identical, the level of
anesthesia can be considered “adequate”.
A slow increase in the difference between the RE and SE values
during anesthesia is a sign of frontal muscle EMG activity, which
in turn is a sign of “inadequate” anesthesia
44.
ENTROPY
AND
ANESTHETIC
DRUGS
The functionality ofthe entropy monitor has been
validated for propofol, thiopental, sevoflurane,
and desflurane anesthesia.
They produce anesthesia by increasing the
activity of GABA-A receptors in the brain
Entropy monitoring is not able to reliably assess
the patient’s depth of anesthesia when
ketamine, xenon or nitrous oxide is used
The entropy indices are found to be less
interfered with the electrocautery unit than BIS
during intraoperative period.
Entropy is also unreliable during high dose
opioid anesthesia.
45.
CONCLUSION
Entropy is avery useful tool for monitoring the depth of anesthesia,
especially in group of patients who may remain too deep or too light
during surgery due to their risk factors.
Because of ease of its usage and numeric interpretation, it has
gained popularity.
It should be kept in mind that the entropy measurement is always to
be used as an adjunct to other physiological parameters.
Objectives
• Onset ofNM Blockade.
• To determine level of muscle relaxation during surgery.
• Assessing patients recovery from blockade to minimize risk of residual
paralysis.
48.
Complications
of residual
paralysis
Respiratory complications
Airwayobstruction
Hypoxia
Aspiration- Residual paralysis can impair pharyngeal
function, which can increase the risk of aspiration
Atelectasis
Pneumonia
Negative pressure pulmonary edema
Other complications
Difficulty in articulation
Delayed extubation
Longer hospital stay
Increased risk of death
49.
History
1958
In 1958, Christieand Churchill-
Davidson described the use of a
nerve stimulator to monitor
neuromuscular block.
1970
However, it was not until the TOF
pattern of stimulation was described
in 1970, that such equipment came
into routine clinical use.
50.
Stimulating the motornerve
The degree of neuromuscular block can be assessed by applying a
supramaximal stimulus to a peripheral nerve, and then measuring
the associated muscular response.
The nerve chosen to be stimulated must fulfil a number of criteria.
1. It must have a motor element
2. It must be close to the skin
3. Contraction in the muscle or muscle group which the nerve
supplies must be visible or accessible to evoked response
monitoring
51.
Definitions
Threshold current: Itis the lowest current required to depolarize the
most sensitive fibres in a given nerve bundle to elicit a detectable
muscle response.
Maximal current: Current which generate response in all muscle fibre
Supramaximal current: It is approximately 25% higher intensity than
the current required to depolarize all fibres in a particular nerve
bundle. This is generally attained at current intensity 2-3 times higher
than threshold current
52.
Ideal nerve stimulator
Anideal nerve stimulator is battery-powered and can deliver a
constant current
Constant current: The stimulator should be able to deliver a constant
current, up to 80 mA.
Monophasic and square wave pattern
Digital display
Safety features: The stimulator should have safety features like circuit
disconnection alerts, low battery alerts, and impedance alerts.
Multiple stimulation mode
Adjustable stimulus amplitude
53.
Application
Good electrical contactwith
the skin can be established
using ECG electrodes of the
silver/silver chloride variety.
The skin should always be
cleansed adequately before
applying the electrodes.
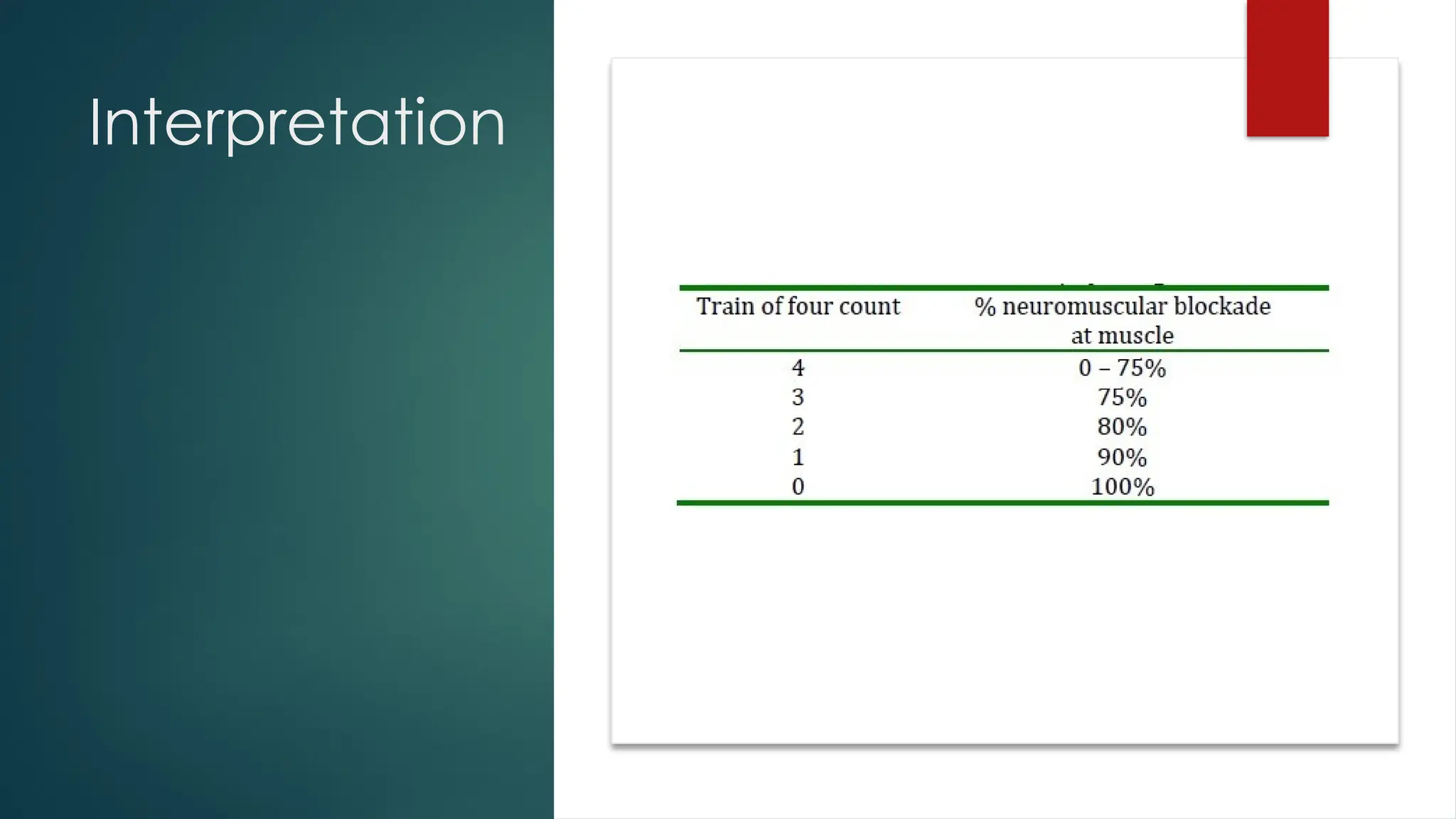
Single twitch
stimulation
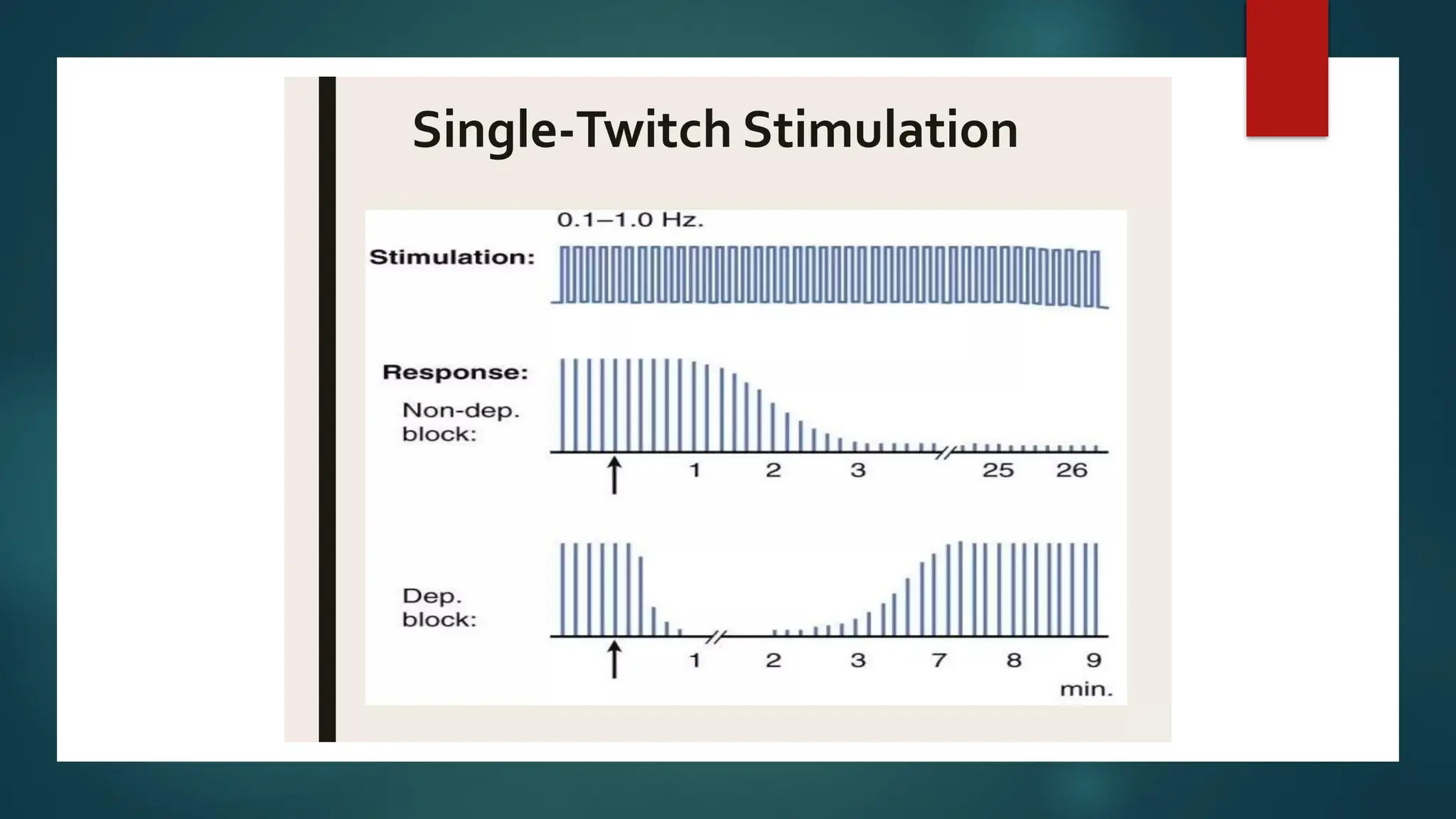
Single squarewave supramaximal stimulus is
applied to a peripheral nerve 1 Hz (1 twitch every
second)to 0.1 Hz (1 twitch every 10second)
Duration of 0.2 ms, at regular intervals and
evoked response is observed
The twitch response will only be depressed when
a neuromuscular blocking agent occupies 75% of
the post-synaptic nicotinic receptors.
Twitch depression will need to be more than 90%
in order to provide good conditions for abdominal
surgery.
57.
Train of four
The TOF pattern of twitch
stimulation was developed to
produce a pattern of stimulation
that did not require the
comparison of evoked responses
to a control response obtained
prior to administration of a
neuromuscular blocking drug.
This requires stimulating the nerve
with supramaximal twitch stimuli,
with a frequency of 2 Hz, that is,
four stimuli each separated by
0.5s and repeated every 10s.
58.
Train of Four
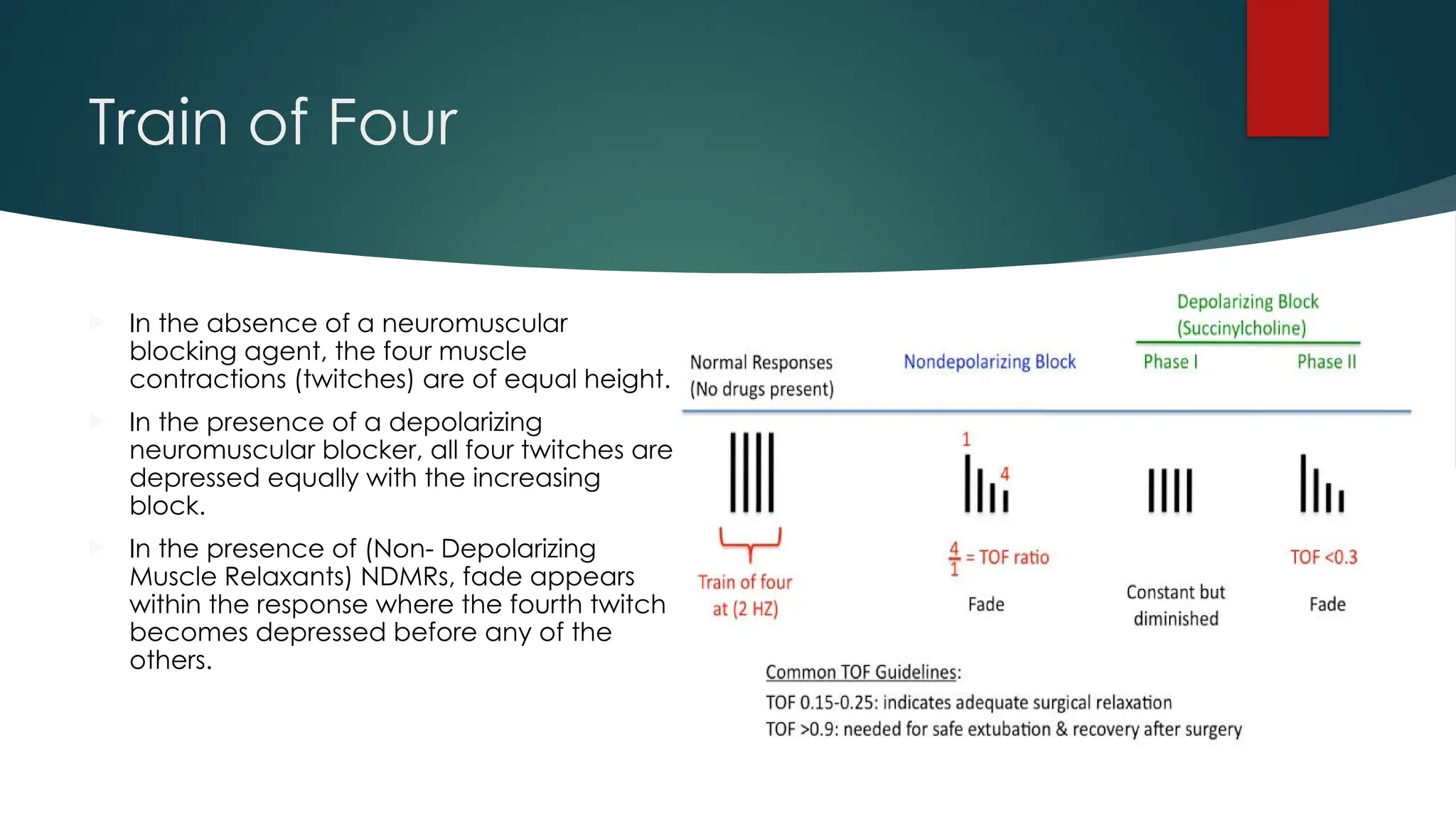
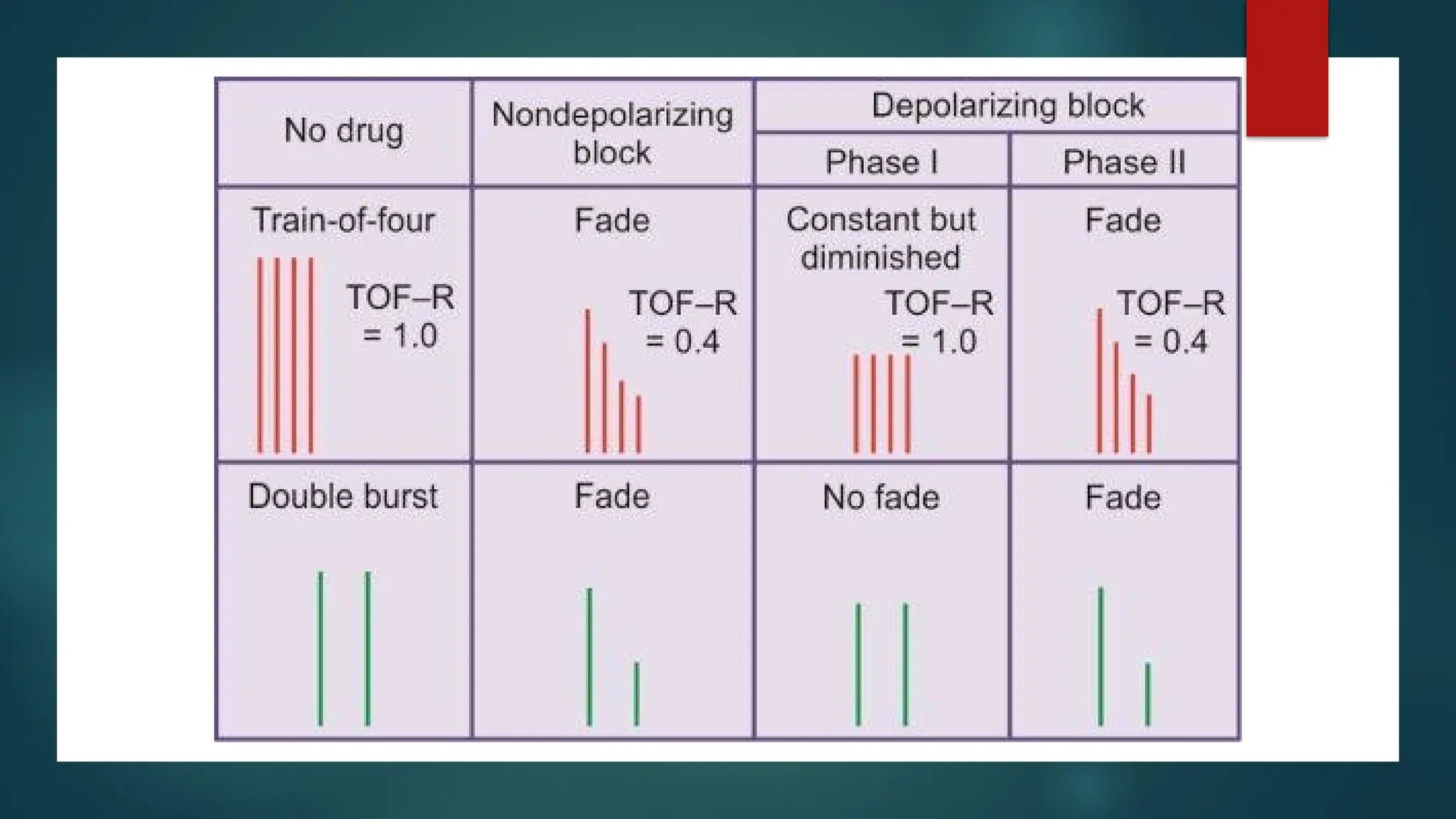
In the absence of a neuromuscular
blocking agent, the four muscle
contractions (twitches) are of equal height.
In the presence of a depolarizing
neuromuscular blocker, all four twitches are
depressed equally with the increasing
block.
In the presence of (Non- Depolarizing
Muscle Relaxants) NDMRs, fade appears
within the response where the fourth twitch
becomes depressed before any of the
others.
Tetanic stimulation
Tetanicstimulation uses a high frequency (50–200 Hz) with
a supramaximal stimulus for a set time: normally 5s.
In healthy skeletal muscle during normal movement, the
response is maintained as a tetanic contraction.
However, on the administration of NMBAs, the muscle,
depending on the degree of block, will show signs of
fade.
At stimulation frequency of 50 Hz the degree of fade will
correspond more closely to the degree of neuromuscular
block.
This pattern of stimulation is very sensitive and can elicit
minor degrees of neuromuscular block, which is
potentially useful in the postoperative recovery room.
However, its use is limited by the fact that titanic
stimulation is extremely painful.
61.
Post tetanic count
During profound non-depolarizing neuromuscular block, there may
be no response to TOF or single twitch stimulation.
If a 5 s tetanic stimulus at 50 Hz is administered, after no twitch
response has been elicited, followed 3 s later by further single
twitches at 1 Hz, there may be a response to single twitch
stimulation.
This pattern will not be seen during very profound block, a response
will be seen in the early stages of recovery, before the TOF
reappears. This is known as post-tetanic facilitation.
62.
Post tetanic
Count
Oncompletion of a tetanic stimulus,
acetylcholine synthesis and mobilization
continue for a short period.
As a result there is an increased, immediately
available store of acetylcholine which causes
an enhanced response to subsequent single
twitch stimulation.
The number of post-tetanic twitches is an
indication of when the first twitch of the TOF will
reappear. For instance, the first twitch of the
TOF generally returns with a PTC of 9 when
using atracurium or vecuronium.
The main use of PTC is when profound
neuromuscular block is required, for example,
during retinal surgery, when movement or
coughing could have devastating effects.
63.
Double burst stimulation
DBS was developed to enable the anaesthetist to detect even small degrees
of neuromuscular block clinically.
Significant bursts of tetanus at 50 Hz at a supramaximal current are applied to
a nerve.
each burst will have three impulses lasting 0.2 ms. Each impulse is delivered
every 20 ms and the two bursts are separated by 750 ms
In unparalysed muscle, two separate muscle contractions of equal intensity will
occur.
In muscle partially paralysed with a non-depolarizing agent, the response to
the second burst is reduced. This is the phenomenon of fade.
The ratio of the magnitude of the second stimulus to the first is known as the
DBS ratio. The DBS ratio has very similar properties to TOF Ratio