2. Myocardial infarction (MI)
• Myocardial infarction (MI), colloquially known as "heart
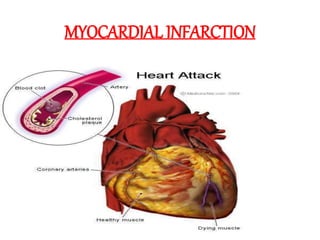
attack," is caused by decreased or complete cessation of
blood flow to a portion of the myocardium.
• Myocardial infarction may be "silent," and go
undetected, or it could be a catastrophic event leading to
hemodynamic deterioration and sudden death.
3. MYOCARDIAL INFARCTION
MI is defined as a diseased
condition which is caused by
reduced blood flow in a
coronary artery due to
atherosclerosis & occlusion of
an artery by an embolus or
thrombus.
MI or heart attack is the
irreversible damage of
myocardial tissue caused by
prolonged ischaemia &
hypoxia.
4. RISK FACTORS
MODIFIABLE RISK FACTORS
• Tobacco use
• High blood cholesterol or Triglyceride levels
• Lack of exercise
• Obesity, Stress
• Lack of daily consumption of fruits or vegetables
• Lack of physical activity
NONMODIFIABLE RISK FACTORS
• Family history
• Older age
• Diabetes
• High blood pressure
8. TYPES OF INFARCTS
1. According to anatomic region of left ventricle invoved:
Anterior
Posterior
Lateral
Septal
Circumferential
Combinations- Anterolateral, Posterolateral, Anteroseptal
2. According to degree of thickness of ventricular wall
involved:
Transmural (full thickness)
Laminar (subendocardial)
3. According to age of infarcts:
Newly formed (acute, recent, fresh)
Advanced infarcts (old, healed, organised)
10. CLINICALMANIFESTATIONS:
• Chest pain / chest discomfort
• Dyspnea
• Fatigue
• Other symptoms include:
Increased sweating
Weakness
Nausea
V
omiting
Light-headedness
Palpitation
•Anxiety, sleeplessness, hypertension or
hypotension, arrhythmia.
•Chest pain is less in women, their common
symptoms are weakness, fatigue & dyspnea.
13. 3.ECG changes:
ST segment
elevation
T wave inversion
appearance of wide deep
Q waves
An elevation of more than
1 mm in contiguous leads is
indicative
15. Management
The key principles that underlie management of myocardial
infarction (MI) include
(1) Minimizing the duration of exposure of myocardium to
ischemia
(2) Rapidly establishing effective reperfusion
(3) Preventing recurrent ischemia and re-occlusion
(4) Managing arrhythmic and mechanical complications
(5) Modifying underlying atherosclerosis toward the aim of
long-term secondary prevention
The targets for therapy are the molecular, cellular, and anatomic
features in the onset, evolution, and complications of MI.
18. Doses for MI
Begin routine medical interventions :
• Supplemental oxygen :6 litres per min for 6 to 12 hours.
• Aspirin:165 -325 mg
• Morphine: 2-4 mg can be repeated 5minutes until pain resolved or
side effects subside.
• Nitroglycerin :sublingual 0.4 mg/5 min for a total of 3 doses in
absence of hypotension.
• If pain not controlled, dose titration can be performed by increment of
19 mcg/5min until pain resolves or heart rate increase or bp decrese
more than 10 %from baseline.
• Thrombolytic (Fibrinolytic) therapy within 90 minutes of hospital
arrival :Streptokinase 1.5 millions unit over 30 -60 minutes.
• Alteplase (tPA):1.5 mg i.v bolus
• 0.75 mg/kg over 30 minutes (upto 50 mg)
• Reteplase (r-PA):10 units +10 units i.v bolus given 30 mins apart
21. Glyceryl Trinitrate (GTN) spray
• Nitroglycerin remains a first-line treatment for angina
pectoris and acute myocardial infarction.
• Nitroglycerin achieves its benefit by giving rise to
nitric oxide, which causes vasodilation and increases
blood flow to the myocardium.
26. Nursing Assessment
One of the most important aspects of care of the patient with MI is
the assessment.
• Assess for chest pain not relieved by rest or medications.
• Monitor vital signs, especially the blood pressure and pulse rate.
• Assess for presence of shortness of breath, dyspnea, tachypnea,
and crackles.
• Assess for nausea and vomiting.
• Assess for decreased urinary output.
• Assess for the history of illnesses.
• Perform a precise and complete physical assessment to detect
complications and changes in the patient’s status.
• Assess IV sites frequently.
27. Nursing management
• Based on the clinical manifestations, history, and
diagnostic assessment data, major nursing
diagnoses may include.
• Ineffective cardiac tissue perfusion related to
reduced coronary blood flow.
• Risk for ineffective peripheral tissue
perfusion related to decreased cardiac output from
left ventricular dysfunction.
• Deficient knowledge related to post-MI self-care
28. Planning & Goals
To establish a plan of care, the focus should be on the following:
Relief of pain or ischemic signs and symptoms.
Prevention of myocardial damage.
Absence of respiratory dysfunction.
Maintenance or attainment of adequate tissue perfusion.
Reduced anxiety.
Absence or early detection of complications.
Chest pain absent/controlled.
Heart rate/rhythm sufficient to sustain adequate cardiac output/tissue
perfusion.
Achievement of activity level sufficient for basic self-care.
29. Nursing Priorities
• Relieve pain, anxiety.
• Reduce myocardial workload.
• Prevent/detect and assist in treatment of life-
threatening dysrhythmias or complications.
• Promote cardiac health, self-care.
30. Nursing interventions
• Administer oxygen along with medication therapy to assist with
relief of symptoms.
• Encourage bed rest with the back rest elevated to help decrease
chest discomfort and dyspnea.
• Encourage changing of positions frequently to help keep fluid
from pooling in the bases of the lungs.
• Check skin temperature and peripheral pulses frequently to
monitor tissue perfusion.
• Provide information in an honest and supportive manner.
• Monitor the patient closely for changes in cardiac rate and rhythm,
heart sounds, blood pressure, chest pain, respiratory status, urinary
output, changes in skin color, and laboratory values.
31. Evaluation
After the implementation of the interventions
within the time specified, the nurse should check if:
• There is an absence of pain or ischemic signs and
symptoms.
• Myocardial damage is prevented.
• Absence of respiratory dysfunction.
• Adequate tissue perfusion maintained.
• Anxiety is reduced.