■ Medical methods:
1. prostaglandins
■ Mifepristone and prostaglandins
■ Gemeprost
■ Dinoprostone
■ Prostaglandin F2 alfa
2.Oxytocin
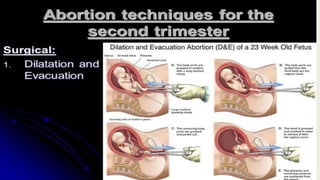
■ Surgical methods:
1. Dilatation and evacuation
2. Intrauterine instillation of hypertonic solution
3. Hysterotomy
4.
Medical methods:
■ Prostaglandins: These are very much effective.
- They are used extensively , specially in 2 nd trimeister.
- They act on cervix and uterus.
- PGE s are prreffered as they have more selective action on
the myometrium and have less side effects.
- MISOPROSTOL( PGE 1 anolog) :400-800mcg of misoprostol
given vaginally at an interval of 3-4 Hrs is most effective as
the bioavailability is high.
-
5.
- Alternativly, firstdose of 600 mcg misoprostol given
vaginally, then 200 mcg, orally every 3 hrs are also found
optimum
- Recently 400 mcg misoprostol is given Sublingually every 3
hrs for a maximum of 5 doses * this regimen got
100%sucess in second trimeister abortion.
6.
■ Mifepristone andprostaglandins – mifepristone 200 mg
oral, followed 36-48 hrs later by misoprostol 800 mcg
vaginal ;then misoprostol 400 mcg oral every 3 hrs for four
is used.
Sucess rate – 97%
Median induction interval – 6.5 hrs.
■ Gemeprost (PGE1 analog) -1 mg vaginal pessary every 3-6
hrs for 5 doses in 24 hrs
Sucess rate - 90%
Median induction interval – 14-18 hrs.
7.
■ Dinoprostone (PGE2 analog) -20 mg is used As vaginal
suppository every
PGE2 is thermo labile, is expensive.
■ Prostaglandin F2 alfa : carboprost -250 mcg IM every 3 hrs
for a maximum 10 doses can be used.
Succes rate -90% in 36 hrs.
S/E ;- nausea, vomiting, diarhoea are more
C/I in bronchial asthma.
9.
2. Oxytocin:
High doseoxytocin is a single agent can be used for second
trimeister abortion. It is effective in 80% of cases. It can be
used with intravenous normal saline along with any other
medications used either intra amniotic or extra amniotic
space in attempt to augment the abortion process.
The drop rate can be increased to 50 milli units or more per
minute .
10.
Surgical methods :
■Between 13 wks and 15 weeks :
dialatation and evacuation :
- in the second trimeister this is less commonly done
- in all mid trimeister abortions cervical preparation must
be used to make process easy and safe.
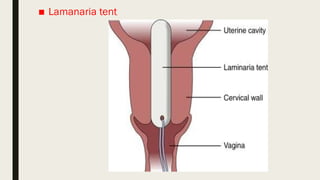
Intracervical tent ( Laminaria osmotic dilator) ,
misoprostol or mifepristone are used as the Cervical priming
agents. The procedure is done under US guidence to reduce
complications.
■ Between 16– 20 weeks : intra uterine instillation of
hypertonic solution
1. Extra amniotic 2 . Intra amniotic
Extra amniotic : Extra amniotic instillation of.0.1 % ethacridine
lactate is done transcervically through No. 16 foleys catheter.
- The catheter passed up the cervical canal for about 10 cm
above the internal OS between membranes and myometrium
and the baloon is inflated with saline. And it is removed after 4
hrs.
Strippimg the membranes with liberation of prostaglandins
from the decidua and dilatation of cervix by the catheter are
some of the known factors for initiation of abortion.
14.
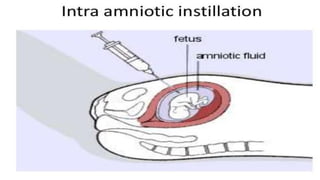
■ Intra amniotic:
Intra amniotic instillation of hypertonic solution is less
commonly used now. It is instilled through abdominal route.
Procedure : preliminary amniocentesis is done with 15 cm 18
gauge needle. The amount of saline to be instilled is calculated
as number of weeks of gestation multiplied by 10 ml. The
amount is to be infused slowly at the rate of 10 ml /min
Contraindications :
Cardiovascular disease
Renal lesion
In severe anemia
15.
Precautions :
1. Tobe sure that needle is in the amniotic cavity evidemced by
clear liquor coming out. If there is bloody tap, the needle
should be pushed further or change the direction until clear
liquor comes out if fails the procedure should be abandoned
2. The instillation should be a slow process
3. Vitals should be monitor. One hour post procedure bed rest is
mandatory.
4. To stop the procedure if the untoward symptoms like acute
abdominal pain, headache, thirst, or tingling in the fingers
appear
A rapid infusion of 1000 ml of dextrose in water along with
intravenous diuretics is indicated in such cases.
16.
5.Strict vigilance istaken during and following
instillation till expulsion occurs.
6. Routine antibiotics given such as ampicillin 500
mg TID for 3-5 days
Mode of action : there is liberation of prostaglandins
following necrosis of the amniotic epithelium and
the decidua. This in turn excites uterine contraction
and results in the expulsion of the fetus.
Sucess rate : 90 -95%
The method failure is considered when abortion
fails to occur within 48 hrs
17.
Complicatipns :
1. Minorcomplications like fever, headache,
nausea,vomitings, abdominal pain
2. Cervical tear and laceration
3. Retained products of conception
4.Infection
5.Hyper natremia – cardio vascualr collapse due to
intravascular injection
6. Pulmonary and cerebral edema
7. Renal failure
8. Disseminated intravascualar coagulation
18.
■ Intra amnioticinstillation of hypertonic urea : i
Intra amniotic instillation of 40% urea solution (80g of urea in
200 ml. Distilled water)
Along with syntocin drip is effective with less complications
■ Hysterotomy : the operation is performed through
abdominal route
Indications : 1.prior failed medical termination of pregnancy
2. Cases where D&E can’t be done safely
Like – fibroid in lower uterine segment
- uterine anomalies
- patient with repeated scarred uterus like placenta
percreta, accreta
* It is less common, always combined with sterilization.
20.
Complications of MTP:
■ Immediate
■ Remote
■ Immediate : - injury to cervix
-uterine perforation during d&E
- Hemorrhage and shock due to trauma, incomplete abortion,
atonic uterus
- Thrombosis and embolism
- Postabortal triad pain, bleeding and low grade fever
Related o methods employed
1. Prostaglandins – intractable vomiting, diarhoea, fever, uterine
pain, cervico uterine injury
2. Oxytocin – water intoxication, convulsions ( rare)
21.
■ 3. Saline: hypernatremia, pulmonary edem, endotoxic shock, D. I. C.,
renal failure
■ Remote :
1. Gynecological – menustrual disturbences
Chronic PID
Infertility due to cornual block
Scar endometriosis
Secondary amenorhea due to uterine synechiae.
2. Obstetrical - recurent mid trimeister abortion due to cervical
incompetence
- ectopic pregnancy , preterm labour, dysmaturity,
increased perinatal loss, rupture uterus, Rh iso immunization in Rh – ve
women, failed abortion and continued pregnancy.
22.
■ Mortality :5-6 times higher chances of mortality is seen in
second trimeister abortions.
■ Rh negative women : in non immunized women ,
intramuscular administration of 100 mcg anti D
immunoglobulin is given within 72 hrs of abortion.



































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

