INTRODUCTION
o Monitoring isimportant to
prevent complications
o Not only about instrumetations
o Anesthesiologists- essential
expertise and interpretations to
monitoring beyond
instrumentation
5.
ASA STANDARDS FORBASIC ANESTHETIC
MONITORING
o STANDARD I
Qualified anesthesia
personnel shall be present
in the room throughout
the conduct of all general
anesthetics, regional
anesthetics and monitored
anesthesia care.
o STANDARD II
o Oxygenation
o Ventilation
o Circulation
o Temperature
6.
BASIC MONITORING
CLINICAL MONITORING
1.PULSE RATE
2. COLOR OF SKIN
3. BLOOD PRESSURE
4. INFLATION OF CHEST
5. PRECORDIAL AND ESOPHAGEAL
STETHOSCOPY
6. SIGNS OF SYMPATHETIC OVER ACTIVITY
7. URINE OUTPUT (>0.5ML/MIN)
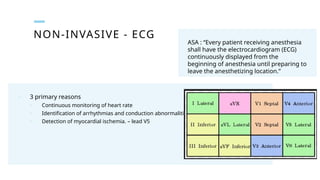
NON-INVASIVE - ECG
ASA: “Every patient receiving anesthesia
shall have the electrocardiogram (ECG)
continuously displayed from the
beginning of anesthesia until preparing to
leave the anesthetizing location.”
o 3 primary reasons
o Continuous monitoring of heart rate
o Identification of arrhythmias and conduction abnormalities – lead II
o Detection of myocardial ischemia. – lead V5
11.
NON-INVASIVE
BLOOD PRESSURE
(NIBP)
o Thecuff must also be snugly fitted and measure
40% of arm circumference and 80% of length of
the upper arm.
o Cuff that is too large falsely low readings
o Cuff that is too small falsely high readings
12.
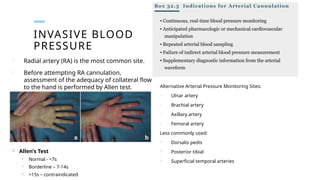
INVASIVE BLOOD
PRESSURE
o Radialartery (RA) is the most common site.
o Before attempting RA cannulation,
assessment of the adequacy of collateral flow
to the hand is performed by Allen test. Alternative Arterial Pressure Monitoring Sites:
o Ulnar artery
o Brachial artery
o Axillary artery
o Femoral artery
Less commonly used:
Dorsalis pedis
Posterior tibial
Superficial temporal arteries
Allen’s Test
Normal - <7s
Borderline – 7-14s
>15s – contraindicated
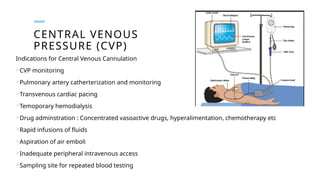
16.
CENTRAL VENOUS
PRESSURE (CVP)
Indicationsfor Central Venous Cannulation
CVP monitoring
Pulmonary artery catherterization and monitoring
Transvenous cardiac pacing
Temoporary hemodialysis
Drug adminstration : Concentrated vasoactive drugs, hyperalimentation, chemotherapy etc
Rapid infusions of fluids
Aspiration of air emboli
Inadequate peripheral intravenous access
Sampling site for repeated blood testing
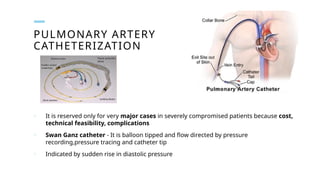
18.
PULMONARY ARTERY
CATHETERIZATION
o Itis reserved only for very major cases in severely compromised patients because cost,
technical feasibility, complications
o Swan Ganz catheter - It is balloon tipped and flow directed by pressure
recording,pressure tracing and catheter tip
o Indicated by sudden rise in diastolic pressure
PULSE OXIMETRY
Click iconto add picture
o OXYGEN SATURATION – SPO2
o NORMAL SPO2 - 97 – 98 %
o PROBE IS APPLIED AT :
o finger
o nail bed,
o toe nail bed ,
o ear lobule,
o tip of nose
o USES : DETECTION OF HYPOXIA
INTRA/POST OPERATIVE
Errors in :
• Carboxyhaemoglobinemia
• Methhemoglobinemia
• Anemia
• Hypovolemia and vasoconstriction
• Nail polish
• Shivering
• spO2 below 60%
• Skin pigmentation
• Dyes
21.
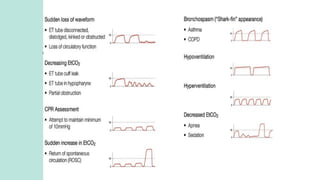
CAPNOGRAPHY
Click icon toadd picture o IT IS THE CONTINUOUS MEASUREMENT
OF END TIDAL (EXPIRED) CARBON
DIOXIDE (ETCO2) AND ITS WAVEFORM.
o NORMAL: 32 TO 42 MMHG (3 TO 4
MMHG LESS THAN ARTERIAL PCO2
WHICH IS 35 TO 45 MMHG).
o PRINCIPLE : INFRARED LIGHT
ABSORBED BY CARBON DIOXIDE
o IMPORTANT AND SENSITIVE
MONITORING
OTHERS
Click icon toadd picture
o LUNG VOLUMES – SPIROMETER
o OXYGEN ANALYSERS
o Monitor actual value oxygen delivered
o Fitted in inspiratory in limb of breathing
circuit
o Useful in closed circuit (use low flow oxygen)
o AIRWAY PRESSURE MONITORING
o It should less than 20 – 25cm H2O
o Low pressure – disconnection
o High pressure – obstruction in tube or
circuit and bronchospasm
25.
APNEA MONITORING
(MONITORING OFRESPIRATION)
Click icon to add picture
o APNEA IS CESSATION OF RESPIRATION FOR MORE THAN 10S.
INTUBATED PATIENTS
o CAPNOGRAPHY - MOST SENSITIVE AND COST EFFECTIVE TO
DETECT APNEA
o AIRWAY PRESSURE MONITOR
NON INTUBATED PATIENTS
o MONITORING THE AIRFLOW AT NOSTRILS (ACOUSTIC PROBE)
o DETECTION OF CHEST MOVEMENTS
Impedence plethysmography – chest is encircled by a coil
Transthoracic impedence pulmonometery
FOR INTUBATED AND NON INTUBATED PATIENT
o PULSE OXIMETER
26.
MONITORING BLOOD LOSS
Clickicon to add picture o ESTIMATION OF BLOOD LOSS IS DONE BY WEIGHING
BLOOD SOAKED SWABS, SPONGES (GRAVIMETRIC
METHOD) AND ESTIMATION OF BLOOD LOSS IN
SUCTION BOTTLE (VOLUMETRIC METHOD).
ON AN AVERAGE (A ROUGH GUIDE):
o FULLY SOAKED SWAB MEANS 20 ML OF LOSS.
o FULLY SOAKED SPONGE MEANS 100 TO 120 ML OF
LOSS.
o A FIST OF CLOTS MEANS 200 TO 300 ML OF LOSS.