Download to read offline


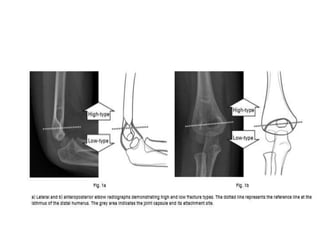





This study investigates the impact of fracture level on the functional outcomes of Gartland type III supracondylar humeral fractures in children managed with closed reduction and percutaneous pinning. It found that fractures below the isthmus of the distal humerus were associated with poorer prognoses, particularly for children aged ten years and older. The research proposes a new subclassification for these fractures to better inform clinical outcomes and perioperative counseling.


































































