Download to read offline
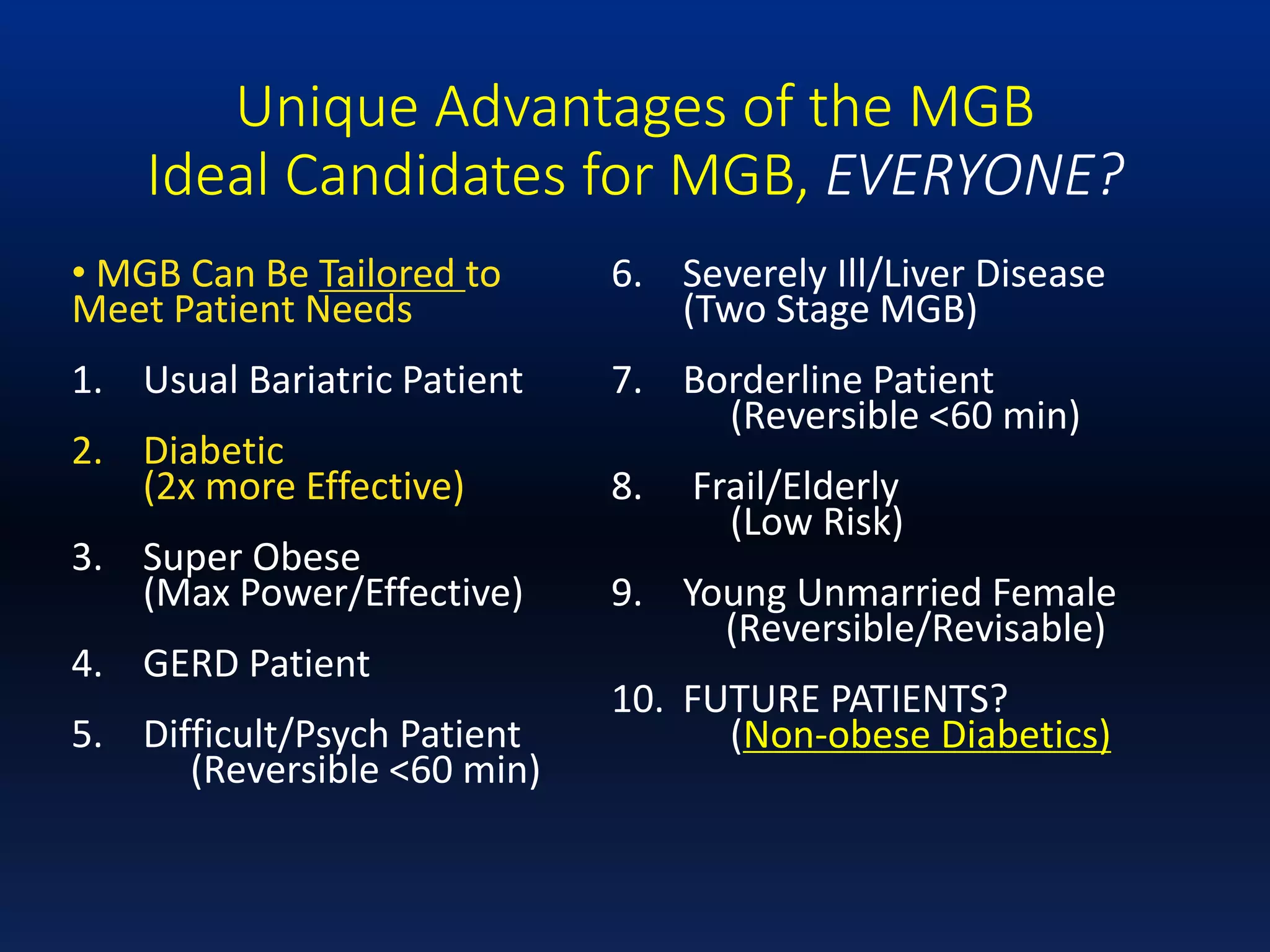
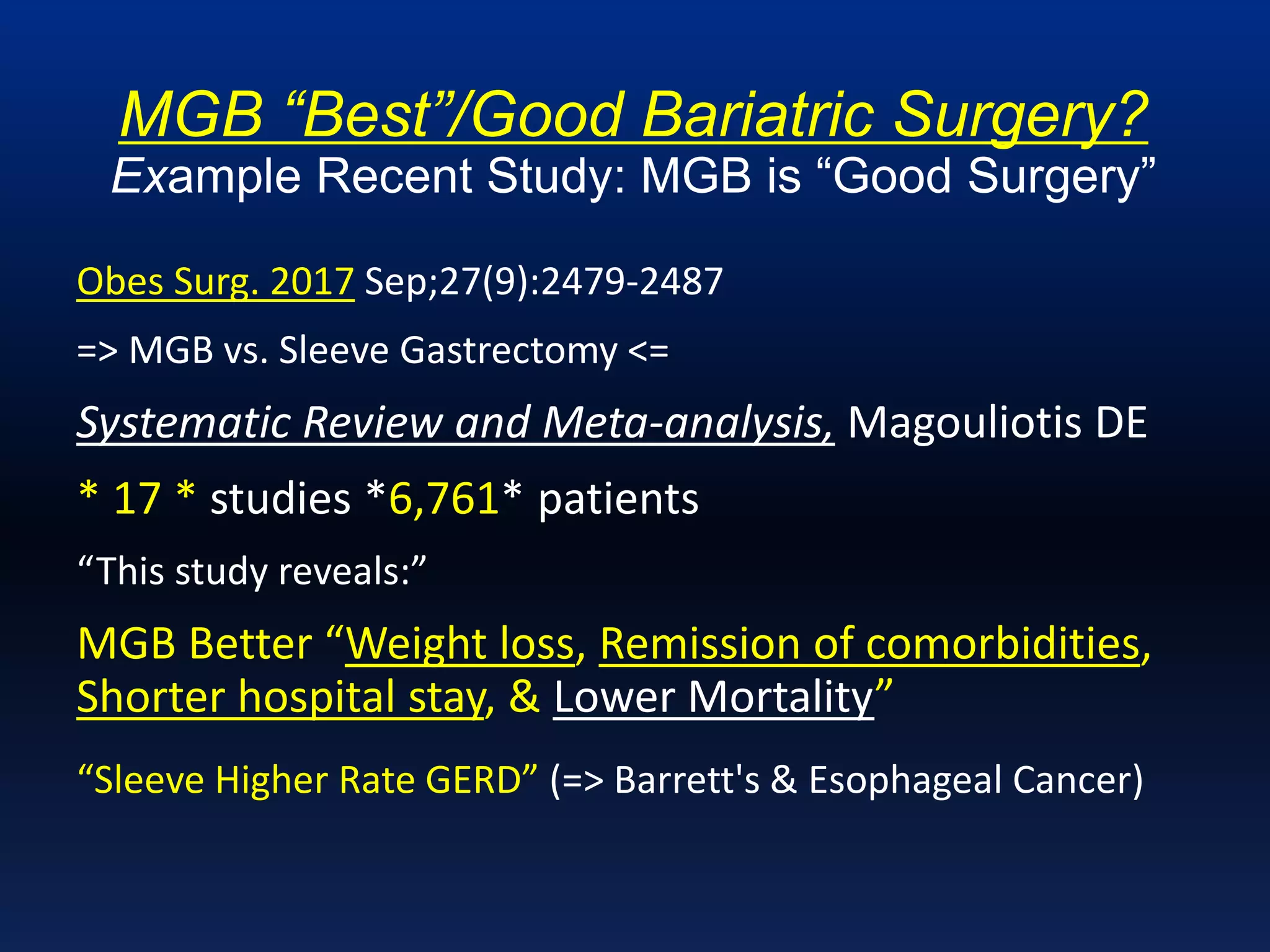











The mini-gastric bypass (MGB) is presented as a highly effective bariatric surgery option, cited to be equal to or better than sleeve gastrectomy and Roux-en-Y in treating obesity and related comorbidities, particularly type 2 diabetes. Multiple studies highlight MGB's advantages such as higher weight loss, lower complication rates, and fewer hospital stays, while also emphasizing the importance of proper technique and understanding to mitigate risks. Despite some controversies and misunderstandings within the surgical community regarding its implementation, MGB is advocated as a safe, simple, and reversible procedure when performed correctly.





















































































