Pharmacist 's workupof drug
therapy (PWDT)
• A tool available to practitioners that serves as a
guide through the steps of the patient care process.
• Contains the thought processes necessary for
pharmaceutical care.
• Helpful to a pharmacy student or a pharmacist
entering a new field of pharmacy practice.
• As a training/orientation exercises.
3.
Components of PWDT
FindingsSubjective data /Objective data.
Desired outcomes Assessment.
Drug-related problems Forms the basis for the intervention plan.
Therapeutic selection Resolutions/Recommendation.
Monitoring parameters Plan.
Follow-up.
Patient care process:
1) patient assessment.
2) creation of a pharmaceutical care plan.
3) follow-up evaluation.
SOAP note.
S =
subjective
findings.
Leadsto, the recognition of a pharmacotherapy problem or
Indication.
Subjective data are open to individual interpretation.
Patient 's statement of complaint ( the chief complaint ; cc)
duration/severity of symptoms.
O =
objective
findings.
Leads to, the recognition of a pharmacotherapy problem or
Indication for pharmacist intervention.
objective data are easily duplicated or quantified.
Laboratory data, weight , height , blood pressure, and pulse.
A =
assessment
Physician's working diagnosis.
possible explanations for the patient 's medical problem(s) .
pharmacist 's evaluation of the subjective and objective findings.
P =
plan.
Physician's intended drug regimen(s), surgical procedures, and/or
diagnostic tests.
pharmacists may not have the authority to initiate/alter drug
therapy regimens.
Monitoring and follow-up.
6.
CORE pharmacotherapy plan3
C=
condition
patient need.
include nonmedical
conditions/needs.
O =
outcome(s)
desired for the conditions or
needs.
1) Patient outcomes
(POEMS: patient -oriented evidence that
matters) .
(2) Therapeutic end points
(DOES: disease-oriented evidence)
R =
regimen
to achieve the desired
outcome.
Therapeutic regimens.
Goal setting and behavior regimens.
E =
evaluation
parameters
to assess outcome
achievement .
Efficacy parameters.
To ensure that therapeutic end points or
patient outcomes are being achieved.
Toxicity parameters.
To ensure that adverse effects, allergic
reactions, or toxicity is not occurring.
7.
Patient outcomes----Dr LawrenceWeed
POEMS: patient -oriented evidence that
matters.
Five categories of patient outcomes:
– Mortality
– Morbidity
( i ) Related to disease process
( ii ) Related to medication/ treatment plan
– Behavior.
– Economic,
– Quality of life.
8.
POMR components
•1. Thedefined data base
•2. The complete problem list
•3. The initial plan
•4. The progress notes
9.
Therapeutic end points
(DOES:disease-oriented evidence):
• Pharmacological/therapeutic effect that is
expected to achieve the desired outcome(s) .
• More than one end point is usually needed to
achieve an outcome.
10.
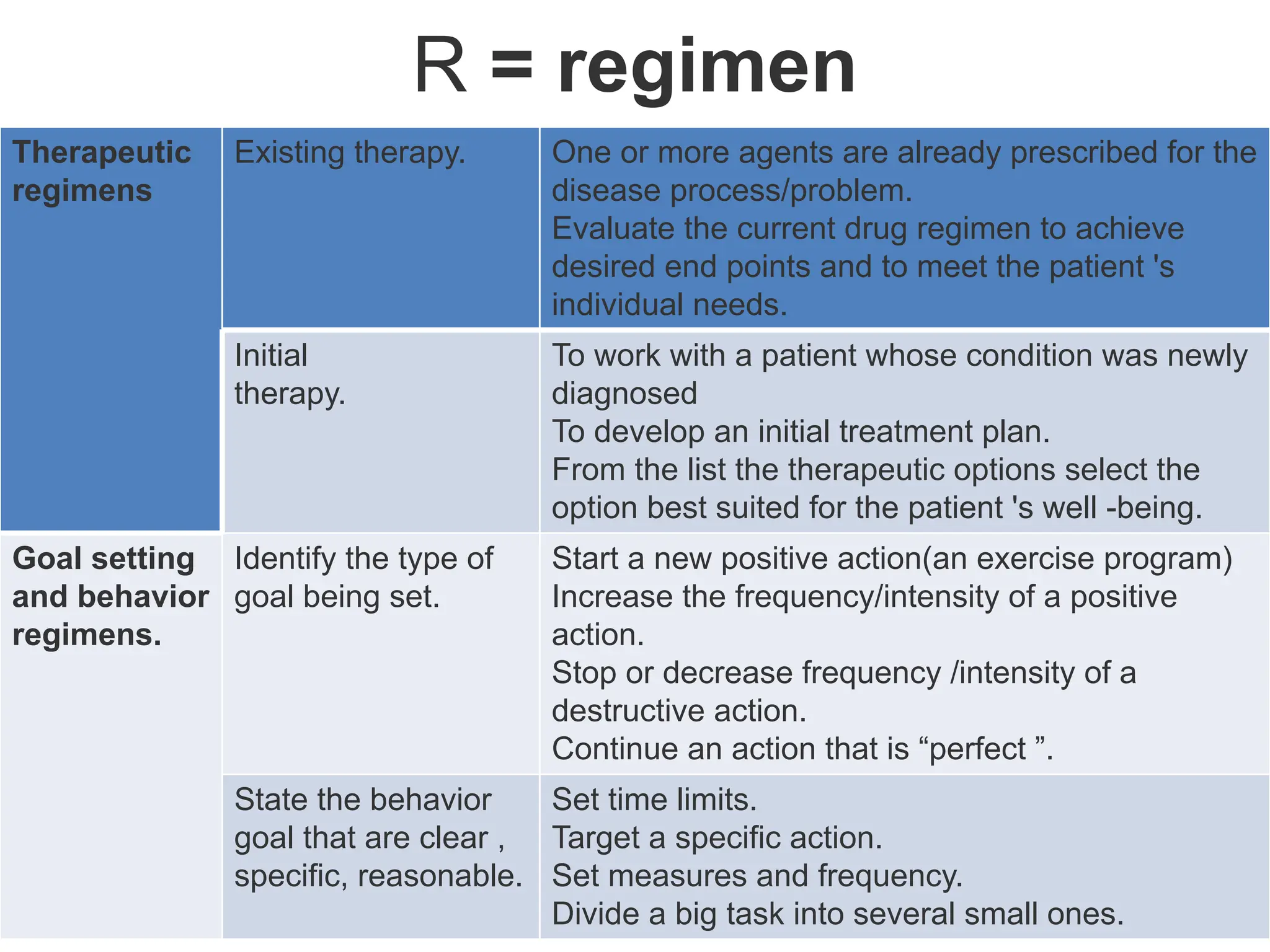
R = regimen
Therapeutic
regimens
Existingtherapy. One or more agents are already prescribed for the
disease process/problem.
Evaluate the current drug regimen to achieve
desired end points and to meet the patient 's
individual needs.
Initial
therapy.
To work with a patient whose condition was newly
diagnosed
To develop an initial treatment plan.
From the list the therapeutic options select the
option best suited for the patient 's well -being.
Goal setting
and behavior
regimens.
Identify the type of
goal being set.
Start a new positive action(an exercise program)
Increase the frequency/intensity of a positive
action.
Stop or decrease frequency /intensity of a
destructive action.
Continue an action that is “perfect ”.
State the behavior
goal that are clear ,
specific, reasonable.
Set time limits.
Target a specific action.
Set measures and frequency.
Divide a big task into several small ones.
11.
PRIME pharmacotherapy problems
•Referred to as drug-related problems.
• Goal is to identify actual or potential problems that
could compromise the desired patient outcomes.
P = Pharmaceutical-based
problems
Patient not receiving a prescribed drug, device, or intervention
Routine monitoring (labs, screenings, exams) missing
R = Risks to patient Adverse drug reaction/drug allergy.
I = Interactions Drug-drug, drug-disease, drug-food interactions
M = Mismatch between medications and condition or patient needs
No indication for a current drug.
Indication for a drug, device, or intervention but none prescribed
E = Efficacy issues Too much of the correct drug
Too little of the correct drug
Wrong drug, device, intervention, or regimen prescribed.
More efficacious choice possible
Canaday BR, Yarborough PC. Documenting pharmaceutical care: Creating a standard. Ann Pharmacother 1994;28:1292-
1296.
12.
FARM note
F =
findings.
patient-specific
information
leads to, the recognition of a pharmacotherapy problem or
indication.
findings include subjective and objective Information.
A =
assessment
Evaluation of
the findings
To make recommendations.
Severity/priority/urgency of the problem.
Short - term and long- term goals of the intervention.
R =
resolution
intervention
plan
Actual or proposed actions by the pharmacist.
Recommendations to other healthcare professionals.
Rationale for choosing a specific intervention should be
stated.
d. M =
monitoring
follow-up. To assess the efficacy, safety, and outcome of the
intervention.
The parameter to be followed? e.g pain, depressed mood.
The intent of the monitoring? e.g efficacy, toxicity,
How the parameter will be monitored? e.g. patient interview.
Frequency of monitoring.
Duration of monitoring.
desired outcome? e.g. , no pain.
Decision point to alter therapy? (e.g. , pain still
present after 3 days.
13.
pharmaceutical care
“pharmaceutical careis the responsible provision of drug therapy for the purpose of
achieving definite outcomes that improve a patient’s quality of life.”
(Hepler and Strand in 1990)
Desired outcomes of pharmaceutical care
1) Cure of a patient’s disease.
2) Reduction or elimination of disease symptoms;
3) arresting or slowing progression of a disease;
4) Preventing a disease or symptoms.
5) To reduce drug-related morbidity and mortality.
6) Address all the patient’s drug-related needs.
7) Establish a caring therapeutic relationship with individual patients.
Patients must receive the most appropriate, effective, safe, convenient, and economical
therapy.
To identify, resolve, and prevent drug therapy problems.
To ensure that optimal patient outcomes are achieved.
14.
Monitoring of Pharmacotherapeuticplan
• Drug therapy problems:
Undesired outcomes associated with drug therapy.
A.
Pharmaceutical care plan.
To increase the frequency and benefits of desired outcomes.
1. Assessment. to determine the need for medication.
2. Plan. based on the assessment of the patient
3. Monitoring. review of the outcomes of drug therapy.
B.
Drug therapy problems
less-than-optimal drug therapy.
1. Unnecessary drug therapy.
2. Wrong drug.
3. Dose too low.
4. Adverse drug reaction.
5. Dose too high.
6. Inappropriate adherence.
7. Need additional drug therapy.
15.
Monitoring therapy
• Patientswith renal or hepatic impairment.
• Close monitoring is required
– for medicines with narrow therapeutic indices.
– for the subset of drugs where therapeutic drug monitoring
may be beneficial
for example, digoxin,
• phenytoin, theophylline and aminoglycosides.
Anticoagulant therapy, including warfarin and
unfractionated heparin.
16.
Steps to Intervention
(1)Observing/reassessing/following no intervention necessary at this time.
(2) Counseling or educating the patient or caregiver
(3) Making recommendations to the patient or caregiver and prescriber.
(4) Informing the prescriber About the recommendations made.
(5) Withholding medication or advising against use.
17.
PHARMACIST'S ROLES IN
PHARMACEUTICALCARE.
Role Skills Required
A. Patient
assessment
Physical assessment
Barriers to adherence
Psychosocial issues
B. Patient
education
and
counseling
empathy, listening, speaking or
writing at the patient 's level of
understanding.
Ability to motivate, inspire
Develop and implement a patient
education plan
resolution of compliance barriers
Interview skills
Communication skills
C. Patient –
specific
pharmacist
care plans
Recognition, prevention, and
management of drug interactions.
Interpretation of laboratory tests.
Pharmacology and
therapeutics.
Professional referrals
Communication.
D. Drug-
treatment
protocols
Update protocols.
Monitor aggregate adherence to
treatment protocols
Drug-use evaluations;
DUEs.
18.
E. Dosage
adjustment
Risk forexaggerated or
sub-therapeutic response.
pharmacokinetic principles
interpret relevant tests
assess dosage adjustment
F. Selection of
therapeutic
alternatives
Use drug information resources
Review and critique drug
literature.
G. Preventive
services
Immunizations
Screenings
19.
Drug use process(DUP) indicators
Need for a drug Ensure there is an appropriate indication for each drug.
all medical problems are addressed therapeutically
Select drug With consideration of patient variables, formulary status and cost of
therapy.
Select regimen most appropriate drug regimen at the least cost.
Provide drug Facilitate the dispensing and supply process.
Drugs are accurately prepared, dispensed in ready-to administer
Form.
Delivered to the patient on a timely basis.
Drug
administration
Appropriate devices and techniques are used for drug administration
Monitor drug
therapy
For effectiveness or adverse effects.
To determine whether to maintain, modify or discontinue.
Counsel patient To ensure proper use of medicines
Evaluate
effectiveness
20.
IMPORTANCE OF
PHARMACEUTICAL CARE
•Use of prescription and nonprescription
medications is growing.
• Complexity, and potency of prescription and
nonprescription drug products are increasing.
• Secures an enduring role for the pharmacist in
healthcare system.
• Integrate pharmacists into the healthcare
system of the future.
21.
Follow up
Resolved
-the goalshave been achieved and therapy is completed.
Stable
-the goals have been achieved, but continue the same therapy.
Improved
-progress is being made toward achievement of the goals, so continue the same therapy.
Partial improvement
-progress is being made, but minor adjustments in the therapy are required.
Unimproved
-there is no measurable progress yet, but continue the same therapy.
Worsened
-there is a decline in health, so revise the therapy accordingly.
Failure
-the goals are not achievable with the present therapy, so initiate new therapy.
Expired
-the patient died while receiving drug therapy.
(Encyclopedia of Clinical Pharmacy)
22.
Mnemonics (Roger Walker)
WWHAMWho is it for?
What are the symptoms?
How long has it been going on?
Action taken?
Medicines taken?
AS
METTHOD
Age of the patient?
Self or for someone else?
Medicines being taken?
Exactly what do you mean (by the symptom)?
Time and duration of the symptom
Taken any action (medicine or seen the doctor)?
History of any disease?
Other symptoms?
Doing anything to alleviate or worsen the symptom?
ENCORE Evaluate the symptom.
No medication is always an option.
Care when dealing with specific patient groups.
Observe the patient for signs.
Refer when in doubt.
Explain any course of action recommended.
23.
Relevant patient details(Roger Walker)
Age Very young and the very old are most at risk of medication-related
problems.
Gender Prompt consideration of the potential for pregnancy or breast
feeding.
Ethnic or
religious
background
Racially determined predispositions to intolerance or ineffectiveness.
Formulations may be problematic for other groups
Social history Living alone or in a care home or availability of nursing, social or
informal carers?
Presenting
complaint
Might be attributable to the adverse effects of prescribed or
purchased medicines.
Working
diagnosis
To identify the classes of medicines that would be anticipated on the
prescription based on current evidence.
Previous medical
history
Guides the selection of appropriate therapy.
Laboratory or
physical
findings
Focus should be on findings that may affect therapy.
Results may convey a need for dosage adjustment.
Presence of an adverse reaction.
24.
Medication history
• Identifyany allergies or serious adverse
reactions.
• medicines in the patient's possession.
• generic name of medicine, dose, frequency,
duration of therapy.
• inhalers, eye drops, topical medicines, herbal
and homeopathic remedies.
• swallowing difficulties.
• ability to read labels.
• Supply problems.
25.
Good Reads
• Comprehensive_Pharmacy_Reviewby shargel Pharmaceutical
Care and Disease State Management Peggy C. Yarborough
• Roger Walker.
• Gennaro AR Remington----Documenting, Billing, and
Reimbursement for Pharmaceutical Care Services Michael T
Rupp.C H A P T E R 117
• Gennaro AR Remington---- Development of a Pharmacy Care
Plan and Patient Problem Solving Deepika Vadher, PharmD,
BCPS Bradley C Cannon, PharmD C H A P T E R 122