Download to read offline

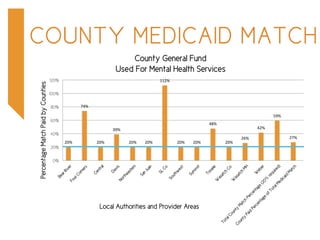


The report outlines the financial structures and challenges faced by local mental health authorities in Utah, particularly regarding Medicaid funding and county matching requirements. It highlights the shift from a fee-for-service system to a capitated Medicaid system, the resultant savings, and the need for ongoing Medicaid match funding to support behavioral health services. There is a call for an additional $6.4 million in ongoing Medicaid match funds for the 2016 legislative session to address growing service demands.






















































































