Download to read offline

![complex reorganization of how Couper’s prac-
tice operates. The practice has reorganized itself
into what Martin’s Point calls a “care team” that
includes a physician, a nurse, a medical assis-
tant, and a patient service representative. The
care team meets weekly to devise strategies for
the patients it has identified as needing extra
support, and quarterly to review the entire pa-
tient pool and see if others need to be given extra
attention. This is made possible by the electronic
health records that Martin’s Point began adopt-
ing in 2005 and by analysis provided by the sys-
tem’s fourteen-person informatics team.
Martin’s Point president and chief executive
officer David Howes says that two particular fea-
tures distinguish the new approach. “The physi-
cian and the rest of the care team feel a respon-
sibility for the care of a population of patients,”
he says, while they also try to anticipate the pop-
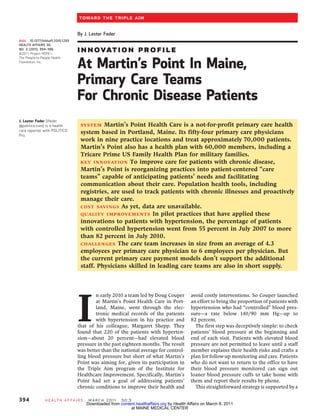
Physician Alain Montegut and medical assistant Maria Gleason, members of a Martin’s
ulation’s care needs. This change in provider
Point Health Care team, examine a patient at the Martin’s Point Portland, Maine, health
mind-set is complemented by “patient-friendly center. The teams are designed to improve care of chronically ill patients by anticipating
processes that are utilized to engage the pa- their needs and coordinating their treatment.
tient,” such as following up by phone.
Couper’s team far exceeded the goal of control-
ling blood pressure in 82 percent of patients with strategies to improve management of their con-
hypertension, reaching 88 percent. Similar re- ditions. In the hypertension program, for exam-
sults were achieved in a parallel project run by ple, patients who are not coming in to have their
another Martin’s Point physician, Margaret blood pressure monitored may be loaned a blood
Shepp. The results from these pilots have been pressure cuff and asked to call the office with
so strong that other Martin’s Point doctors are their results.
adopting them, and innovation is spreading Providing patients with such simple ways to
through the organization “just by osmosis,” take control of their own care can have a dra-
Howes says. matic effect, Couper says. He gave the example of
one patient who had been using a loaner cuff
who started off with blood pressure readings
Care Teams And Chronic Disease of 224/98. Today he’s down to 152/76 and is
A key to success has been careful efforts to design saving up to buy a cuff of his own.
and build the care teams and provide them with Couper is now preparing to expand his model
ongoing support. The system has found that to target cholesterol. Just under two-thirds of the
teams work best when headed by a strong physi- patients in his practice have a low-density lip-
cian-leader who can direct their vision and allo- oprotein level under 100; he’s now aiming for
cate resources appropriately. vastly more to have their cholesterol controlled.
Also critical is equipping the team with tools to Hanging on his office wall is a classic “fish-
assess its patient population—including an over- bone” or Ishikawa diagram from the quality im-
all information infrastructure that can give the provement movement listing impediments to pa-
team usable data on patients’ health, as well as a tients’ ability to manage their cholesterol. These
routine for reviewing the data and adjusting the include transportation difficulties that keep pa-
practice to improve outcomes. Physicians and tients from making appointments, failure to fol-
other medical staff also receive additional com- low prescribed diets, insurance issues such as
pensation for training in the use of electronic gaps in coverage, and process issues such as
health records and registries for recording and whether patients come in for routine checkups.
analyzing population health data. Then the team starts identifying where addi-
Creating registries spotlights gaps in patient tional interventions can be most effective.
care, showing that “docs do a very good job tak-
ing care of patients who come in on a regular
Photo: Kevin Bruise
basis” but not with those “who don’t come in [or] Financing
who don’t take their medicine,” Couper says. The Better management of chronic conditions may
team regularly meets to review the files of pa- help patients avoid costly hospitalizations and
tients who are having difficulty and try to identify other interventions, but they are not cost-free. As
M a r ch 2 0 1 1 30:3 H e a lt h A f fai r s 395
Downloaded from content.healthaffairs.org by Health Affairs on March 8, 2011
at MAINE MEDICAL CENTER](https://image.slidesharecdn.com/martinspointchronicdiseasemodel-110314084528-phpapp02/85/Martins-point-chronic-disease-model-3-320.jpg)
![Toward The Triple Aim
Martin’s Point continues to reorganize around
the care team model, the system will need to Providing patients
increase the average number of nurses and other
employees per primary care physician from 4.3
with simple ways to
to 6. “That will allow them to see more patients
[, and] it will allow them to be far more effective
take control of their
in the care of the populations,” Howes says. But own care can have a
the additional staff time is not directly reimburs-
able under a fee-for-service model that rewards dramatic effect.
“production” rather than population health
management, he adds. “The revenue streams
are simply not there, and the business models
that we need to support that are not preeminent
in our community,” he says.
However, through its own health plan, Mar- tions will persuade others to adopt their model.
tin’s Point is already moving to build the new In the meantime, other findings have surfaced.
payment model. It has adopted a system of cap- “An unexpected group of frontline physicians
itation, in which its doctors will be paid almost have become very interested” in the notion of
double if they simultaneously achieve higher pa- boosting patients’ confidence and self-efficacy
tient confidence, better quality, and lower total to deal with their conditions, Howes says. And
cost for care. The system is also exploring mov- recruiting more doctors committed to the new
ing physicians to some version of a salaried sys- model is a challenge: “We really need primary
tem with incentives for quality improvement. care clinicians interested in, and excited about,
Howes and other Martin’s Point officials hope leading care teams.” ▪
that results from their pilot and similar innova-
This paper was commissioned by Health Delivery, December 16, 2010, in innovations_across_the_nation_in_health_
Affairs and is based partly on a Washington, D.C. For a copy of the care_delivery/2010_12_16_innovations_
presentation by David Howes, Martin’s agenda and a full list of conference across_the_nation_in_health_care_
Point Health Care, that was delivered at sponsors, please visit http:// delivery.php.
a Health Affairs conference, Innovations www.healthaffairs.org/
across the Nation in Health Care issue_briefings/2010_12_16_
396 Health A ffairs M a r c h 20 1 1 30 : 3
Downloaded from content.healthaffairs.org by Health Affairs on March 8, 2011
at MAINE MEDICAL CENTER](https://image.slidesharecdn.com/martinspointchronicdiseasemodel-110314084528-phpapp02/85/Martins-point-chronic-disease-model-4-320.jpg)

Martin's Point Health Care in Maine implemented patient-centered "care teams" to improve management of chronic conditions like hypertension. The teams, composed of a physician, nurse, medical assistant and patient representative, meet weekly to coordinate patient care. They use population health tools to proactively manage patients and anticipate their needs. In pilots, the percentage of patients with controlled hypertension increased from 55% to over 82% after implementing care teams. However, primary care payment models do not support the larger staff required for care teams.






























































![Va pcmh study 6 2014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/vapcmhstudy620141-140801153322-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































