Downloaded 10 times


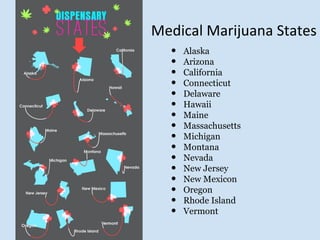

The document is a brief guide outlining marijuana state laws and federal regulations, listing states where medical marijuana is legal. It highlights specific states such as California, Arizona, and New Jersey among others. For further details, it references an infographic and historical context provided through external links.






















![Legalizing Marijuana[1]](https://cdn.slidesharecdn.com/ss_thumbnails/legalizingmarijuana1-090511160050-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














