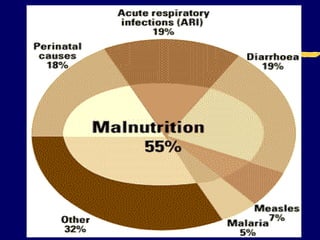
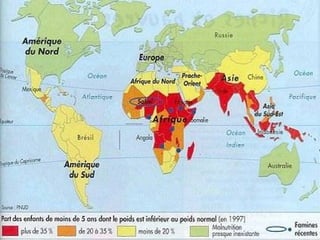
This document discusses protein energy malnutrition (PEM), including its causes, types, assessment, and treatment. PEM is caused by inadequate intake of protein and calories and is highly prevalent in developing countries, contributing to over 50% of deaths in children under 5. The two main types of PEM are kwashiorkor, characterized by edema, and marasmus, characterized by wasting. PEM is assessed through clinical exam, anthropometry, dietary assessment, and laboratory tests. Treatment involves rehydration, dietary supplementation, infection treatment, and prevention of complications. PEM has severe health impacts and early detection and management are important for recovery.