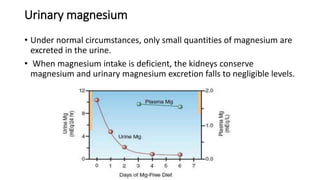
This document discusses electrolyte imbalances related to magnesium. It begins by describing magnesium's role in over 300 enzyme reactions and its importance for muscle and nerve function. It then details normal magnesium distribution and regulation, factors that increase or decrease magnesium levels, signs of hypermagnesemia and hypomagnesemia, and treatment approaches for correcting magnesium imbalances.

![Plasma Magnesium Concentration
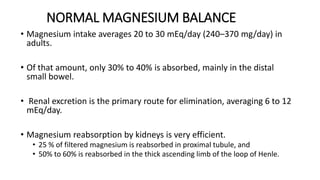
• Plasma [Mg 2+ ] is closely regulated between 1.7 and 2.1 mEq/L (0.7–1
mmol/L or 1.7–2.4 mg/dL) through interaction of
• Gastrointestinal tract (absorption)
• Bone (storage), and
• Kidneys (excretion)
• Approximately 50% to 60% of plasma magnesium is unbound and
diffusible.](https://image.slidesharecdn.com/magnesiumjyothibose-240401061024-c991a9d8/85/MAGNESIUM-JYOTHIBOSE-pptx-deficiency-disorder-10-320.jpg)
![HYPERMAGNESEMIA
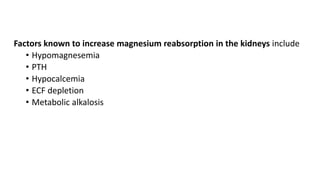
• Hypermagnesemia (serum Mg >2 mEq/L)
• Increases in plasma [Mg 2+ ] are nearly always due to excessive intake
(magnesium-containing antacids or laxatives: magnesium hydroxide,
Milk of Magnesia), kidney impairment (GFR<30ml/min) or both.
• Magnesium sulfate therapy for preeclampsia and eclampsia can result in
maternal and fetal hypermagnesemia.](https://image.slidesharecdn.com/magnesiumjyothibose-240401061024-c991a9d8/85/MAGNESIUM-JYOTHIBOSE-pptx-deficiency-disorder-11-320.jpg)






























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















