Recommended

Recommended
More Related Content
What's hot
What's hot (19)
Similar to Lutheran Research Fair-- Random Glucose All-Cause Mortality [Autosaved]
Similar to Lutheran Research Fair-- Random Glucose All-Cause Mortality [Autosaved] (20)
Lutheran Research Fair-- Random Glucose All-Cause Mortality [Autosaved]
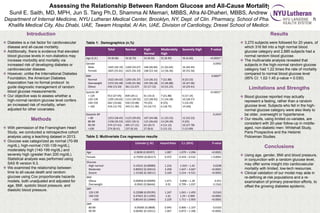
- 1. Assessing the Relationship Between Random Glucose and All-Cause Mortality Sunil E. Saith, MD, MPH, Jun S. Tang Ph.D, Shamma Al Memari, MBBS, Afra Al-Dhaheri, MBBS, Andrew Kohut, MD, MPH Department of Internal Medicine, NYU Lutheran Medical Center, Brooklyn, NY, Dept. of Clin. Pharmacy, School of Pharmacy, UCSF, Sheikh Khalifa Medical City, Abu Dhabi, UAE, Tawam Hospital, Al Ain, UAE, Division of Cardiology, Drexel School of Medicine, Philadelphia, PA Introduction Diabetes is a risk factor for cardiovascular disease and all-cause mortality. Additionally, there is evidence that elevated blood glucose levels in non-diabetics may increase morbidity and mortality via increased risk of developing diabetes or cardiovascular disease. However, unlike the International Diabetes Foundation, the American Diabetes Association has no formal protocol to guide diagnostic management of random blood glucose measurements. Our objective was to assess whether a high-normal random glucose level confers an increased risk of mortality, when adjusted for other covariates. Methods With permission of the Framingham Heart Study, we conducted a retrospective cohort analysis using a teaching dataset in 2013. Glucose was categorized as normal (70-99 mg/dL), high-normal (100-139 mg/dL), moderately high (140-199 mg/dL) and severely high (greater than 200 mg/dL). Statistical analysis was performed using SAS ® version 9.3. We examined the relationship between time to all-cause death and random glucose using Cox proportionate hazards models, both unadjusted and adjusted for age, BMI, systolic blood pressure, and diastolic blood pressure. Results 3,270 subjects were followed for 20 years, of which 316 fell into a high normal blood glucose category and 2,885 subjects had a normal random blood glucose. The multivariate analysis revealed that subjects in the high-normal random glucose category had 1.22 times the rate of mortality compared to normal blood glucose level (95% CI: 1.02-1.45 p-value = 0.030). Limitations and Strengths Blood glucose reported may actually represent a fasting, rather than a random glucose level. Subjects who fell in the high- normal glucose category were also likely to be older, overweight or hypertensive. Our results, using limited co-variates, are consistent with 20-year follow-up in middle- aged, non-diabetic men: Whitehall Study, Paris Prospective and the Helsinki Policeman Studies. Conclusions Using age, gender, BMI and blood pressure, in conjunction with a random glucose level, may offer some insight into cardiovascular mortality with limited, low-tech resources. Clinical validation of our model may aide in re-defining at-risk populations and a re- examination of primary prevention efforts, to offset the growing diabetes epidemic. Total Normal High- Normal Moderately High Severely High P-value Age (S.D.) 50 (8.68) 50 (8.70) 52 (8.50) 55 (8.90) 56 (6.60) <0.0001* Gender Male Female 1445 (44.19) 1825 (55.81) 1260 (43.67) 1625 (56.33) 148 (46.84) 168 (53.16) 21 (63.64) 12 (36.36) 16 (44.44) 20 (55.56) 0.0992 BMI Normal Overweight Obese 1422 (44.02) 1372 (42.48) 436 (13.50) 1293 (45.37) 1196 (41.96) 361 (12.67) 114 (36.31) 145 (46.18) 55 (17.52) 7 (21.88) 15 (46.88) 10 (31.25) 8 (23.53) 16 (47.06) 10 (29.41) 0.0007* Systolic BP < 120 120-139 140-159 > 160 913 (27.95) 1295 (39.65) 642 (19.66) 416 (12.74) 839 (29.1) 1151 (39.92) 550 (19.08) 343 (11.90) 61 (19.3) 123 (38.92) 79 (25) 53 (16.77) 7 (21.88) 11 (34.38) 8 (25) 6 (18.75) 6 (17.14) 10 (28.57) 5 (14.29) 14 (40) <0.0001* Diastolic BP < 80 80-89 90-99 >100 1253 (38.45) 1158 (35.53) 574 (17.61) 274 (8.41) 1123 (39.05) 1021 (35.5) 495 (17.21) 237 (8.24) 107 (34.08) 115 (36.62) 65 (20.7) 27 (8.6) 11 (33.33) 13 (39.39) 4 (12.12) 5 (15.15) 12 (33.33) 9 (25) 10 (27.78) 5 (13.89) 0.2437 Table 1: Demographics (n,%) Estimate (+ SE) Hazard Ratio C.I. (95%) P-value Age 0.0838 (0.00397) 1.087 1.079 – 1.096 <0.0001 Female -0.75055 (0.06117) 0.472 0.419 – 0.532 < 0.0001 Glucose High normal Moderate Severe 0.19531 (0.08989) 0.89922 (0.20414) 1.15182 (0.18211) 1.216 2.458 3.164 1.019 – 1.45 1.647 – 3.667 2.214 – 4.521 0.0298 <0.0001 <0.0001 BMI Obese Overweight 0.06858 (0.09099) -0.0942 (0.06644) 1.071 0.91 0.896 – 1.28 0.799 – 1.037 0.451 0.1563 SBP 120-139 140-159 >160 0.22088 (0.09195) 0.47621 (0.11295) 0.80143 (0.13484) 1.247 1.61 2.229 1.041 – 1.493 1.29 – 2.009 1.711 – 2.903 0.0163 <0.0001 <0.0001 DBP 80-89 90-99 -0.05685 (0.0808) 0.06481 (0.10311) 0.945 1.067 0.806 – 1.107 0.872 – 1.306 0.0163 <0.0001 Table 2: Multivariate Cox regression results