








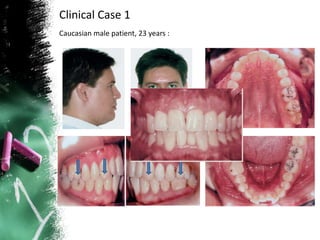

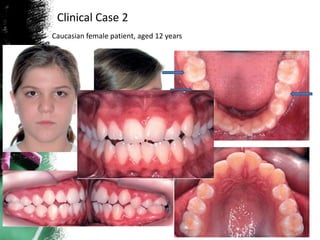





Lower incisor extraction is an orthodontic treatment option for addressing crowding and alignment issues. It provides several advantages, including maintaining arch form, decreasing treatment and relapse time, and improving facial profile and dental occlusion. However, it also carries some risks such as space reopening in the extraction site and compromised dental esthetics. The decision to extract a lower incisor depends on a case-by-case evaluation of factors like arch length discrepancy, anterior tooth ratio, and buccal interdigitation. Clinical cases demonstrate successful resolution of crowding issues through targeted lower incisor extraction.


















































































