Journal of Indianacademy of dental
specialist researchers , 2014
Objective was to evaluate the use of mandibular incisor extraction
in relieving the lower anterior crowding and its advantages and disadvantages.
3.
Introduction
• Compromised orthodontictreatment can bring out perfection
in treatment, provided the result is functionally and
esthetically in harmony for each respective case.
• Neff found that the maxillary anterior teeth are 18-36%
larger than the mandibular anterior teeth.
• He indicated that compensation should be made for
segments that are not in harmony.
• The concept of removing the lower incisor for the purpose of
relieving the crowding was first introduced by Hahn.
4.
• Though thelower incisor extraction is not a
standard approach to symmetrically treating most
malocclusions, in certain clinical situations, the
therapeutic aids must be adjusted to individual
patient needs, even when the achieved final
occlusion is not ideal.
5.
Materials and methods
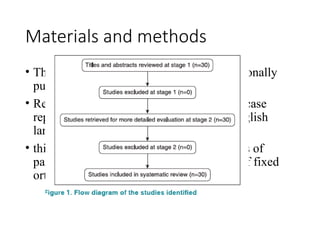
•The search strategies included the internationally
published research.
• Review articles, published bibliographies, case
reports, relevant citations in articles, in English
language were included.
• this review was restricted to clinical studies of
patients who had completed a full course of fixed
orthodontic treatment.
6.
Results
• The onecommon feature between all the
articles cited is that none of the authors have
strictly contraindicated the lower incisor
extraction.
• All use of a diagnostic setup to assess the
outcome of the treatment before doing the
mandibular incisor extraction.
• All the case reports available were with a
minimum of one year post-retention follow-up.
7.
Ideal indications andcase selection for mandibular
incisor extraction
• Class I molar relationship
• A full cusp Class II molar relationship with lower anterior
crowding can also be an ideal case.
• Soft-tissue profile should be normal as there will be minimal
change in the upper arch, which will be an ideal case.
• Minimal growth potential. In growing patients,
nonextraction therapy should be considered.
• Missing lateral incisors or peg laterals, which can solve the
inevitable tooth size discrepancy without any stripping or re-
contouring.
8.
• Class Icases with anterior dental cross-bite, which is due to lower
anterior crowding or lower anterior protrusion can be considered.
• Extreme crowding or protrusion, particularly when accompanied
by gingival recession and bone loss can also be an indication for
lower incisor extraction
• Maxillary dentition with a narrow lateral incisor (measurable
mandibular Bolton excess) may represent good indication for
extraction of one mandibular incisor.
• Cases with borderline Class III or a Class III tendency are also
indicated for lower incisor.
• Tooth Size Arch Length Discrepancy (TSALD) in the mandibular
arch is an indication for extraction of single mandibular incisor,
when there is no adequate space in the arch to accommodate a full
complement of teeth. (TSALD greater than 5 mm in lower
anterior region).
• Presence of deep curve of Spee, proclined lower anteriors where
uprighting can be easily done with a single lower incisor
extraction.
9.
• Extraction oflower incisor is indicated where there
is ectopic eruption and there is presence of normal
intercanine width.
• It is also indicated in cases, where in the final
finishing, when six maxillary anterior teeth are
occluding with five mandibular anterior teeth, an
ideal Class I canine relation is obtained and the
distoincisal inclines of the maxillary canine occlude
with the mesioincisal inclines of mandibular first
premolars.
10.
Advantages of mandibularincisor extraction
• It may reduce the treatment time, if the crowding is
limited to anterior region.
• In case of lower single incisor extraction there is
only a minimal alteration in intercanine width,
which does not pose a threat to the long-term
stability.
• Incisor extraction therapy does not demand much
retraction of the anterior teeth. So the antero-
posterior position of the incisors is not changed
much, allowing the profile to be maintained.
11.
Disadvantages of mandibularincisor extraction
• Overjet increases if there was no Bolton discrepancy
before the start of treatment.
• A Class III occlusal relationship will be the result, if the
overjet is normal after the removal of lower incisor.
• A midline discrepancy is inevitable and there are chances
for extraction space to reopen in the long term.
• As the morphology of the lower incisor are in such a way
that the cervical portion of the crown is narrower
mesiodistally and wider incisally, extracting a single
incisor may lead to sacrifice of inter-dental papilla
leading to ‘black triangle’ formation.
12.
Decision making forwhich incisor to extract
• The critical decision of which lower incisor to extract on
several considerations, including periodontal condition, the
presence of gingival recession and the location of any
restoration, including endodontic treatment.
• Additionally, a mesiodistal width of each incisor should be
measured and the anticipated amount of tooth movement
determined with the Bolton analysis keeping in mind that in
mandible, the central incisors are smaller mesiodistally than
lateral incisor.
• According to Flavio Uribe and Ravindra Nanda, extraction
of a lateral incisor is generally preferred because it is less
visible from the front. But the incisor that is farthest outside
the natural arch and the closest to the crowding is usually the
best tooth for extraction.
13.
Discussion
• Non-extraction therapyin crowded cases is usually
thought to lead to post-retention relapse.
• There was a study involving the evaluation of post-
treatment crowding of mandibular incisors, which
shows that there was no correlation between a change in
the post-retention intercanine width and post-retention
mandibular anterior crowding.
• It is generally agreed that patient treated with the
extraction of four premolars tend to experience a
decrease in mandibular intercanine width and an
increase in incisor irregularity post-retention, regardless
of whether arch width has been expanded or constricted.
14.
• In aneffort to find predictors for the relapse of
mandibular anterior crowding, a study was done to
assess 65 patients, all at least 10-years post-
retention.
• All patients have been treated in permanent
dentition with first premolar extraction. The long-
term response to mandibular anterior alignment was
unpredictable. No variables such as degree of initial
crowding, age, gender, angle’s classification etc.
were useful in establishing the prognosis.
15.
• Seventy percentof patients had unsatisfactory
mandibular anterior alignment in the post-retention
stage. Patients who were slightly crowded before
treatment usually become moderately crowded.
• A review of Edward Hartley Angle’s philosophy of
extraction in Orthodontics, showed that Angle
regarded the extraction of an incisor even when the
tooth was sound.
• Furthermore, Angle warned that extracting one
incisor, as advocated by some, would lead to less
acceptable harmony between the occlusal plane of
the remaining teeth, in addition to an abnormal
incisor overbite.
16.
Conclusion
• Mandibular incisorextraction, as discussed in this
article is a good choice when all the conditions with
regard to its indications are satisfied by a patient.
• Judicious extraction without proper planning should
be avoided, as it may lead to excess overjet,
overbite and occlusion, which are not functionally
stable.
• A proper diagnostic setup is always recommended
before doing mandibular incisor extraction, so that a
proper idea regarding the post-treatment occlusion
can be obtained.
17.
• It isbetter to avoid incisor extraction if the
diagnostic setup does not yield a satisfying post-
treatment occlusion. Otherwise, incisor extraction is
a better choice to opt for, as the mechanics becomes
simpler and good results are achievable.
• Midline compromise will not pose an esthetic
problem as the lower midline is not visible in a
normal social smile.
18.
This systematic reviewaims to assess the stability of treatment results analyzed
by considering parameters like intercanine width and peer assessment rating
(PAR) scores after MIE in orthodontic patients
19.
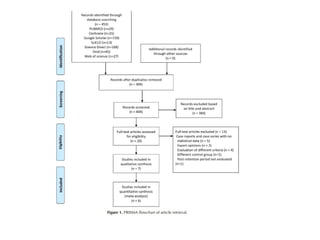
Methodology
• PubMed, CochraneLibrary, Science Direct, Google
Scholar, Ovid, and SciELO were systematically
searched without restrictions in the year of
publication or language up to August 2022.
20.
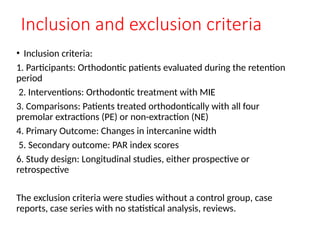
Inclusion and exclusioncriteria
• Inclusion criteria:
1. Participants: Orthodontic patients evaluated during the retention
period
2. Interventions: Orthodontic treatment with MIE
3. Comparisons: Patients treated orthodontically with all four
premolar extractions (PE) or non-extraction (NE)
4. Primary Outcome: Changes in intercanine width
5. Secondary outcome: PAR index scores
6. Study design: Longitudinal studies, either prospective or
retrospective
The exclusion criteria were studies without a control group, case
reports, case series with no statistical analysis, reviews.
21.
• The riskof bias in nonrandomized studies was
assessed using a modified version of the Newcastle-
Ottawa Scale (NOS).
22.
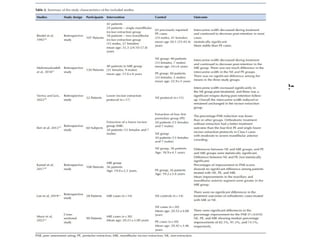
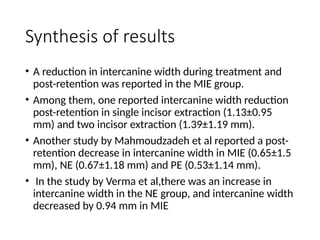
Synthesis of results
•A reduction in intercanine width during treatment and
post-retention was reported in the MIE group.
• Among them, one reported intercanine width reduction
post-retention in single incisor extraction (1.13±0.95
mm) and two incisor extraction (1.39±1.19 mm).
• Another study by Mahmoudzadeh et al reported a post-
retention decrease in intercanine width in MIE (0.65±1.5
mm), NE (0.67±1.18 mm) and PE (0.53±1.14 mm).
• In the study by Verma et al,there was an increase in
intercanine width in the NE group, and intercanine width
decreased by 0.94 mm in MIE
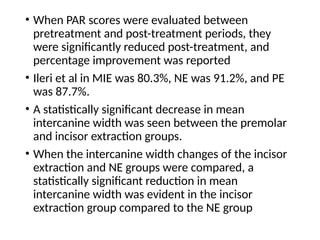
23.
• When PARscores were evaluated between
pretreatment and post-treatment periods, they
were significantly reduced post-treatment, and
percentage improvement was reported
• Ileri et al in MIE was 80.3%, NE was 91.2%, and PE
was 87.7%.
• A statistically significant decrease in mean
intercanine width was seen between the premolar
and incisor extraction groups.
• When the intercanine width changes of the incisor
extraction and NE groups were compared, a
statistically significant reduction in mean
intercanine width was evident in the incisor
extraction group compared to the NE group
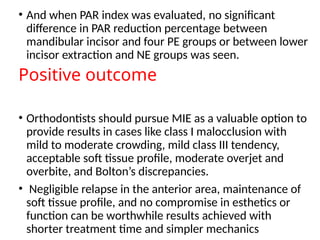
24.
• And whenPAR index was evaluated, no significant
difference in PAR reduction percentage between
mandibular incisor and four PE groups or between lower
incisor extraction and NE groups was seen.
Positive outcome
• Orthodontists should pursue MIE as a valuable option to
provide results in cases like class I malocclusion with
mild to moderate crowding, mild class III tendency,
acceptable soft tissue profile, moderate overjet and
overbite, and Bolton’s discrepancies.
• Negligible relapse in the anterior area, maintenance of
soft tissue profile, and no compromise in esthetics or
function can be worthwhile results achieved with
shorter treatment time and simpler mechanics
25.
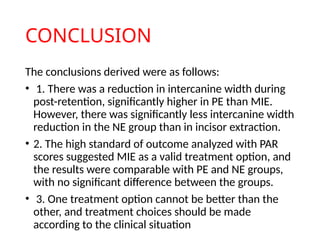
CONCLUSION
The conclusions derivedwere as follows:
• 1. There was a reduction in intercanine width during
post-retention, significantly higher in PE than MIE.
However, there was significantly less intercanine width
reduction in the NE group than in incisor extraction.
• 2. The high standard of outcome analyzed with PAR
scores suggested MIE as a valid treatment option, and
the results were comparable with PE and NE groups,
with no significant difference between the groups.
• 3. One treatment option cannot be better than the
other, and treatment choices should be made
according to the clinical situation
27.
• Extraction ofone mandibular incisor in adolescents and adults
can simplify orthodontic treatment in 2 major circumstances:
(1)Severe crowding of the mandibular but not the maxillary incisors,
(2)Mild anterior crossbite with good alignment in both arches.
• Despite its potential advantages, this method has had limited use
in most practices.
Introduction
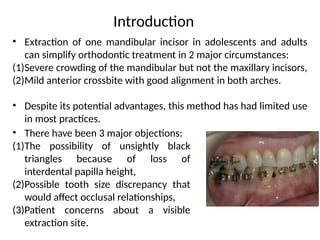
• There have been 3 major objections:
(1)The possibility of unsightly black
triangles because of loss of
interdental papilla height,
(2)Possible tooth size discrepancy that
would affect occlusal relationships,
(3)Patient concerns about a visible
extraction site.
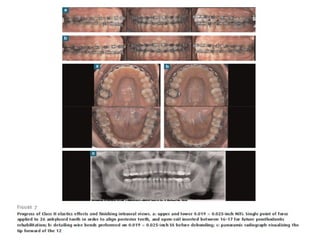
28.
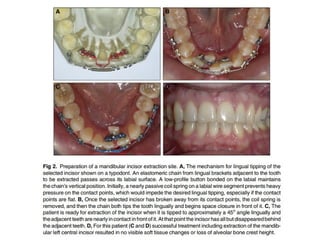
• For 37consecutively treated single-incisor-extraction patients,
preparation of the extraction site was done
• Extraction site preparation is done in 2 steps: first,
orthodontically tipping the incisor that is to be removed lingually
to a safer location for its removal
• Then closing most of the space in front of it before it is extracted.
• For closure of a single mandibular incisor space, elastomeric
chain is the most practical method
• This moves the new extraction site away from the delicate crestal
bone and usually preserves the height of the alveolar crest where
the tooth used to be.
Methods
30.
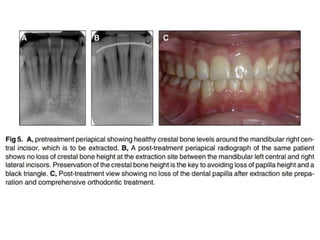
RESULTS
• In patientsbelow age 20, this approach eliminated post-treatment black
triangles and almost eliminated partial loss of the interdental papilla.
• It reduced the previously reported prevalence of these problems in
patients aged 20-40 years and did not seem to be helpful in those aged
over 40 years.
• This positive effect was achieved because of maintenance of alveolar
crest height that supports the interdental papillae.
• Tooth size discrepancy caused by incisor extraction was largely
compensated by the different labio-lingual orientation of maxillary and
mandibular anterior teeth.
• The extraction space quickly disappeared during site preparation.
32.
• The newprocedure of extraction site preparation described in
this paper offers more favorable outcomes for prevention of
post-treatment prevalence of black triangles and loss of
interdental papilla height that could impair dental esthetics in
younger patients but shows limited efficacy in older patients.
• Camouflage of a mild skeletal Class III problem is the major
indication for this extraction pattern.
Conclusions
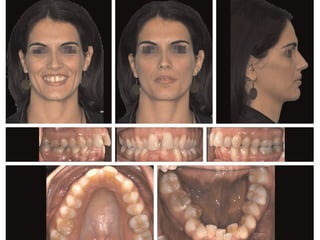
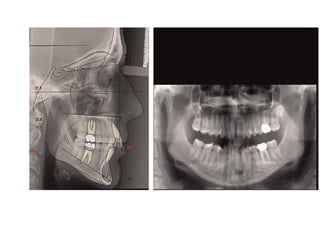
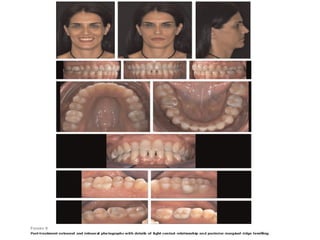
The patient presenteda skeletal Class I with
normodivergent facial pattern, Class II subdivision dental
relationship, extremely deep Curve of Spee and severe
overbite.
Moreover, during the treatment, the upper left first molar
does not respond to orthodontic forces due to tooth
ankylosis, augmenting the
difficulty of this case.
Despite this, a good occlusal relationship on both sites and
an optimal extraoral outcome have been achieved after a
26-months therapy.
40.
Improved smile andlip competency
Partial loss of lower papillae, triangular shape of
lower incisors
Root paralleling without resorption of anteriors
despite considerable intrusion of lower incisors
Reduction in lip protrusion This complex case highlights how
accurate diagnosis, a critical
overview of treatment and good patient compliance are indispensable
factors for achieving good outcomes
TREATMENT RSULTS
CONCLUSION
This complex casehighlights how accurate
diagnosis, a critical overview of treatment and
good patient compliance are indispensable factors
for achieving good outcomes
43.
Objective:
To evaluate thedegree of perception of laypersons, dental
professionals, and dental students regarding dental esthetics in cases
with mandibular central incisor extraction.
44.
• A smilephotograph of a female patient aged 16 years
and 10 months who had normal occlusion.
• The real photograph was manipulated with the aid of
Adobe Photoshop CS3 Software
• Changes in the photograph were made in the region
of the anteroinferior arch of the image with various
compositions of sizes. With the intention of
simulating the extraction of the mandibular right
central incisor, the crown and the gingival curvature
were removed due to the presence of its respective
root.
45.
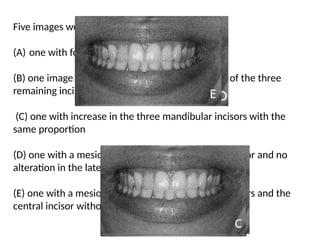
Five images wereobtained:
(A) one with four incisors
(B) one image without any alteration to the width of the three
remaining incisors
(C) one with increase in the three mandibular incisors with the
same proportion
(D) one with a mesiodistal increase in the central incisor and no
alteration in the lateral incisors, and
(E) one with a mesiodistal increase in the lateral incisors and the
central incisor without any alteration
46.
• After manipulationthe images were printed on
photographic paper, attached to a questionnaire and
distributed to laypersons, dental professionals, and
dental students (n 5 90) to evaluate the degree of
perception and esthetic using a scale of
attractiveness, where 0= hardly attractive, 5=
attractive, and 10= very attractive.
47.
Results:
• Photograph Awas scored the most attractive by the three
groups.
• Photograph E was ranked the least attractive by the dental
professionals,
• whereas the dental students and laypersons scored D as
the least attractive photograph.
• Only the grades awarded to photograph A presented
significant differences among the groups.
48.
Conclusions:
It can beconcluded that dental professionals and dental students
are more skillful at identifying deviation from normality.
In addition, central incisor extraction should always be discarded
when there are other treatment options available.
49.
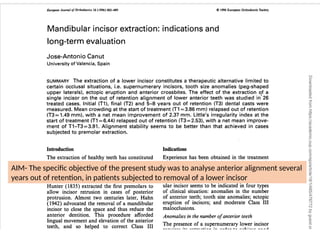
AIM- The specificobjective of the present study was to analyse anterior alignment several
years out of retention, in patients subjected to removal of a lower incisor
50.
INDICATIONS
• The extractionof a mandibular incisor is indicated in four
types of clinical situation: anomalies in the number of
anterior teeth; tooth size anomalies; ectopic eruption of
incisors; and moderate Class III malocclusions.
Anomalies in the number of anterior teeth
• The presence of a supernumerary lower incisor requires its
extraction in order to achieve good occlusal alignment.
• the absence of an upper lateral tooth, may be replaced with
a prosthesis; alternatively, the space can be closed
orthodontically. The extraction of a lower incisor would be
indicated in the latter case, in order to co-ordinate the
occlusion of the incisors
51.
Tooth size anomalies
•Discrepancies in the mesiodistal size of the six anterior teeth
may be corrected by extracting a lower incisor.
• The disproportion, as reflected by Bolton's Index (1958), is
established by the relative macrodontia of the lower incisors,
or microdontia of the upper laterals.
Ectopic eruption of incisors
• The transposition of anterior teeth, particularly of the canines,
or the severe malpositioning of a lower incisor, indicates
extraction to protect the long-term survival of the dentition.
52.
Moderate Class IIImalocclusions
• Anterior crossbite or an edge-to-edge relation of the
incisors with a tendency towards anterior open bite is
another indication for incisor extraction.
• The occlusion improves on shortening the length of the
mandibular arch, which retrudes the position of the lower
incisors
53.
Subjects and methods
•The study sample consisted of 26 patients treated by
Edgewise appliance therapy with extraction of one
mandibular incisor.
• Only cases with plaster models before treatment, at the
time of appliance removal and a minimum of 5 years out of
retention were recorded.
• Digital calipers calibrated to 0.01 mm were used in
measuring all parameters.
54.
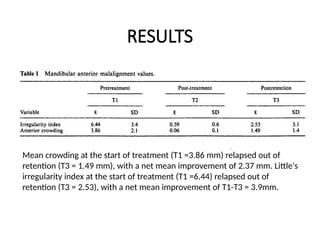
RESULTS
Mean crowding atthe start of treatment (T1 =3.86 mm) relapsed out of
retention (T3 = 1.49 mm), with a net mean improvement of 2.37 mm. Little's
irregularity index at the start of treatment (T1 =6.44) relapsed out of
retention (T3 = 2.53), with a net mean improvement of T1-T3 = 3.9mm.
55.
DISCUSSION AND CLINICAL
IMPLICATIONS
•The extraction of an incisor poses important limitations that
must be taken into account.
• An accentuated overjet is a contra-indication to the removal
of a single lower incisor, closure of the lower space will
increase the overjet.
• On removing an incisor, the canine displaces mesially, and
canine functional protection is lost.
• A diagnostic setup of the final occlusal status must be
evaluated. In certain cases, the space either fails to close or
else opens up with ease; a visible diastema thus results in
an area of considerable aesthetics.
56.
• One wayof preventing relapse is to extract an incisor with
extreme malpositioning, which limits the unnecessary
movement of many teeth
• The loss of gingival tissue or the disappearance of the
external alveolar lamina constitutes an additional indication
for extraction of the affected incisor
Editor's Notes
#12 Contraindications :
Deep bite cases with horizontal G.P. , upper first premolar extraction while canines are in Class I relationship, (3 j
bimaxillary crowding cases which have no tooth-size discrepancy in the incisoox
area, and (4) all cases having incisor discrepancy due to either small lower incisors
and/or large maxillary incisors.