Download to read offline

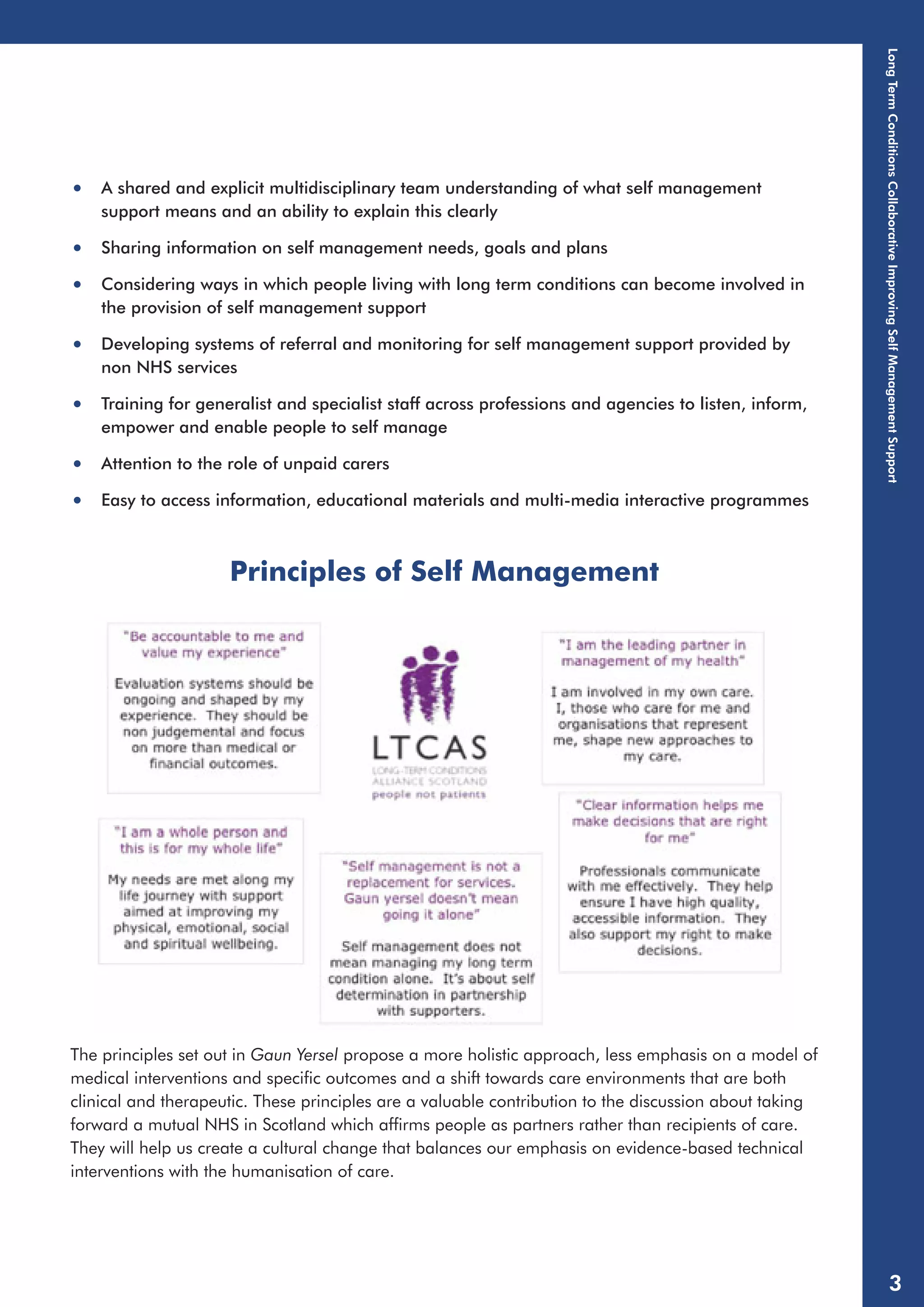
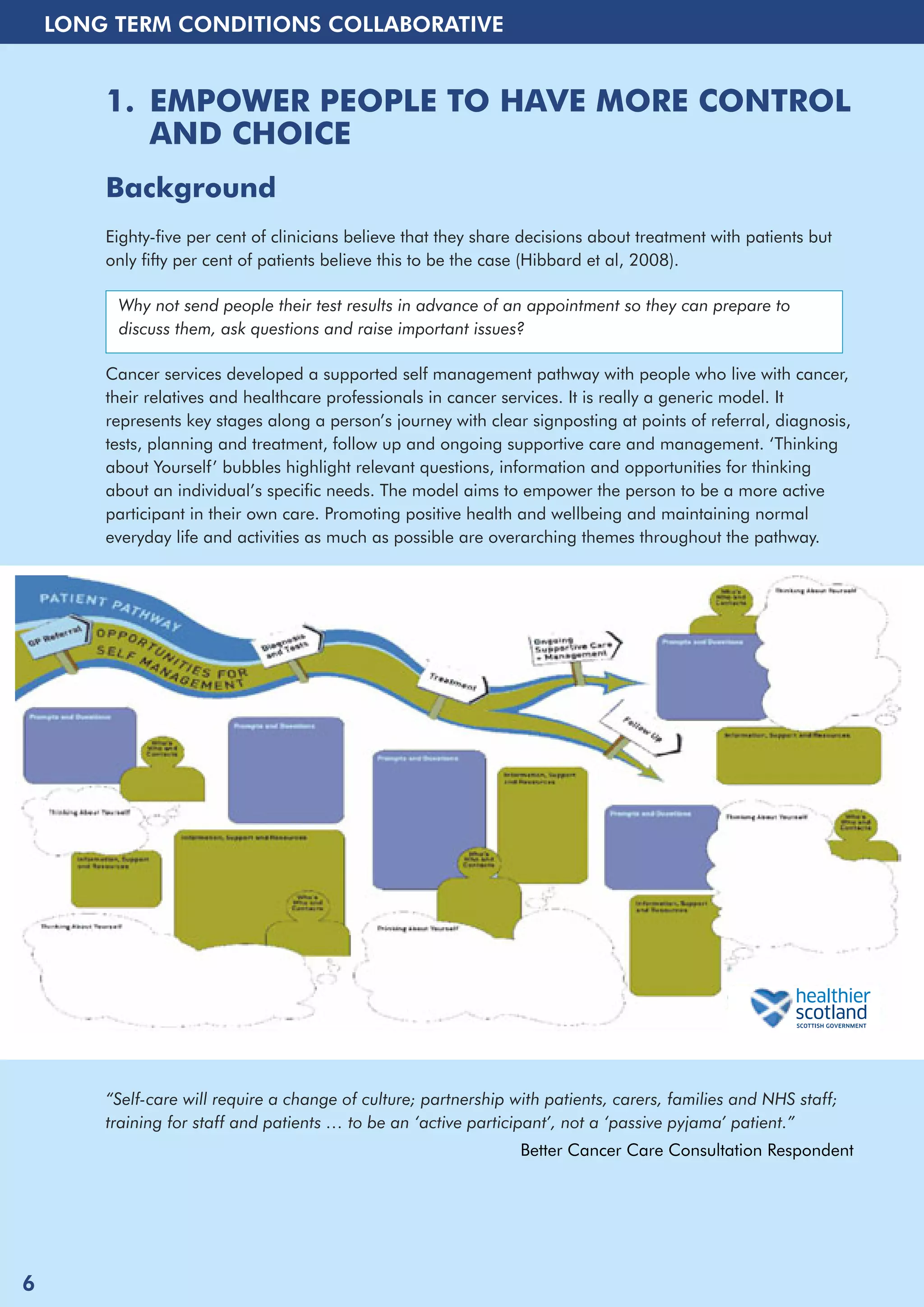

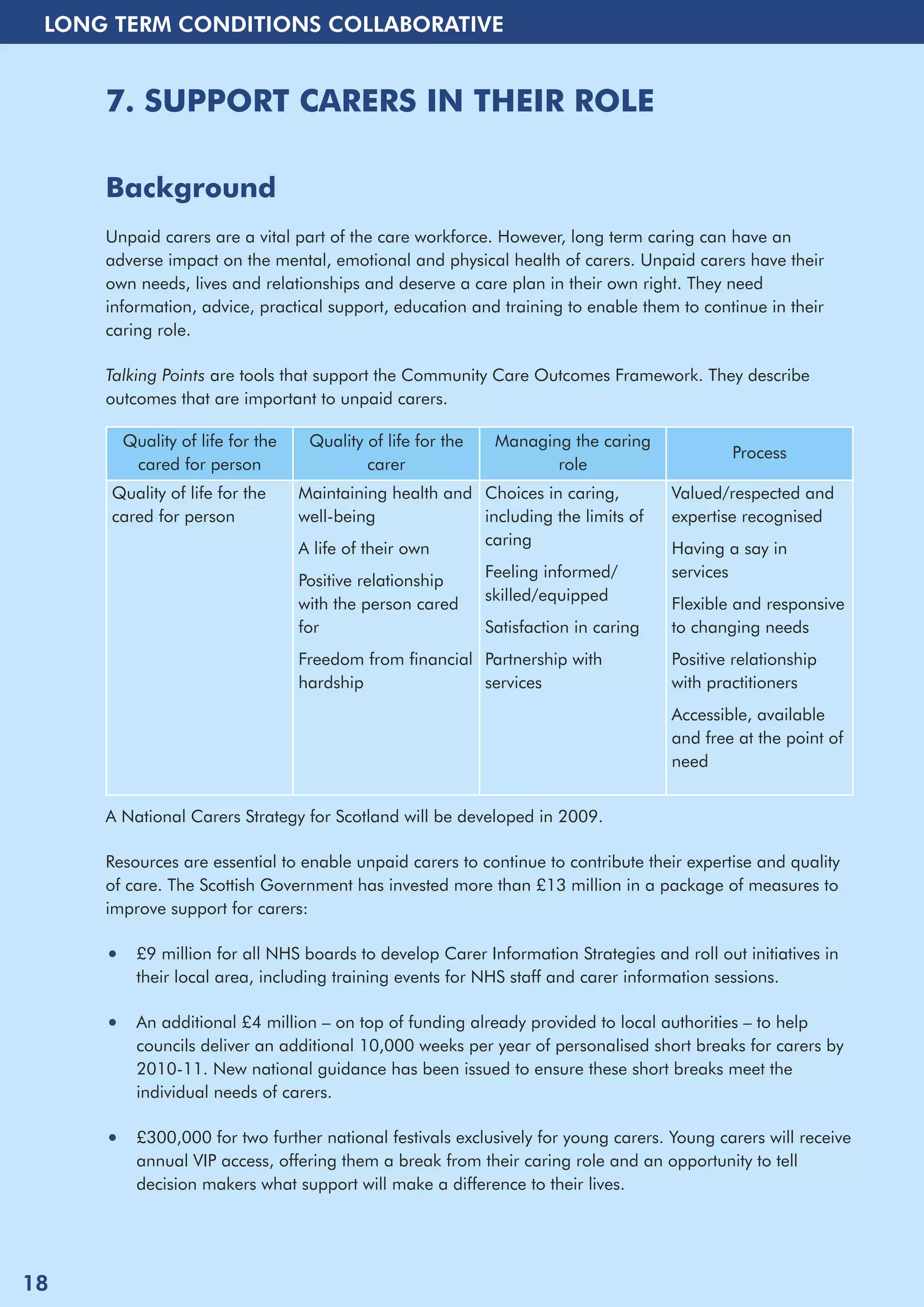

This document provides information and resources to support self-management of long-term conditions in Scotland. It discusses 10 approaches to improving self-management, including empowering people to have more control over their care, promoting better mental health and wellbeing, enabling better access to information and support, developing care plans, supporting medication management, using telehealth, supporting carers, commissioning self-management resources, using patient records, and training staff. For each approach, examples of relevant projects and contacts for additional information are provided. The overall aim is to enhance patient outcomes and experiences by promoting self-management.















































