
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to Long Term Care Needs Evaluation
Similar to Long Term Care Needs Evaluation (20)
Recently uploaded
Recently uploaded (20)
Long Term Care Needs Evaluation
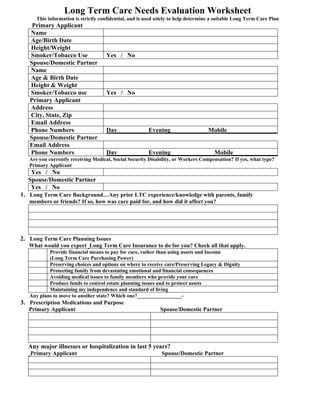
- 1. Long Term Care Needs Evaluation Worksheet This information is strictly confidential, and is used solely to help determine a suitable Long Term Care Plan Primary Applicant Name Age/Birth Date Height/Weight Smoker/Tobacco Use Yes / No Spouse/Domestic Partner Name Age & Birth Date Height & Weight Smoker/Tobacco use Yes / No Primary Applicant Address City, State, Zip Email Address Phone Numbers Day__________Evening____________Mobile________________ Spouse/Domestic Partner Email Address Phone Numbers Day__________Evening______________Mobile_______________ Are you currently receiving Medical, Social Security Disability, or Workers Compensation? If yes, what type? Primary Applicant Yes / No Spouse/Domestic Partner Yes / No 1. Long Term Care Background…Any prior LTC experience/knowledge with parents, family members or friends? If so, how was care paid for, and how did it affect you? 2. Long Term Care Planning Issues What would you expect Long Term Care Insurance to do for you? Check all that apply. Provide financial means to pay for care, rather than using assets and Income (Long Term Care Purchasing Power) Preserving choices and options on where to receive care/Preserving Legacy & Dignity Protecting family from devastating emotional and financial consequences Avoiding medical issues to family members who provide your care Produce funds to control estate planning issues and to protect assets Maintaining my independence and standard of living Any plans to move to another state? Which one?_________________- 3. Prescription Medications and Purpose Primary Applicant Spouse/Domestic Partner Any major illnesses or hospitalization in last 5 years? Primary Applicant Spouse/Domestic Partner
- 2. Any use of mobility aids (walker, wheel chair, power chair, cane) and years of use? Primary Insured Spouse/Domestic Partner Activities Primary Applicant Spouse/Domestic Partner Employed Yes No Employed Yes No Exercise Yes No Exercise Yes No Volunteer Yes No Volunteer Yes No 4. Retirement/Estate Planning Goals to provide for: Self/Spouse Children Charities 5. Any Special Needs Family Members? (Disabilities) What are those needs? Yes No Self Yes No Spouse/Partner Yes No Children Yes No Parents/Siblings 6. Other than current residence, is there any other property involved in estate/retirement planning? Primary Applicant Spouse/Domestic Partner Family Property / Value: $ Value: $ Farm / Value: $ Value: $ Rental Property / Value: $ Value: $ Commercial / Value: $ Value: $ 7. Financial Considerations How are you currently prepared to pay for Long Term Care? Income, Assets, Retirement Portfolio Medical (Do you qualify?) Long Term Care Policy Have you looked at Long Term Care Insurance prior to this time? Yes___ No____ Primary Spouse/Partner Over Under Over Under If asset protection is a concern/priority Are assets you wish to protect over or under $750,000? If under, are total assets you wish to protect over $250,000? If under $250,000 how much of that do you wish to protect? Income Protection Primary Applicant Spouse/Domestic Partner Monthly Income $ $ Pension/Social Security $ $ Retirement Portfolio $ $ 8. For Federal Tax purposes, are you a business owner? Yes No If yes, what type of business? Primary Insured Spouse/Domestic Partner Sole Proprietor S Corp LLC / LLP C Corp
- 3. 2008 Nursing Home Costs in California 2008 Nursing Home Costs in California Daily and Annual Average Rates for a Daily and Annual Average Rates for a Private Room Semi-Private Room $274 / $100,010 $189 / $68,985 2008 Assisted Living Costs in Calif. 2008 Home Health Care Costs in Calif. Monthly and Annual Average Rates Home Health Aide/Certified Nursing $3,663 / $43,956 Assistant and LPN Hourly Rates HHA or CNA Hourly Rate $21 LPN Hourly Rate $51 These figures are part of a 2008 Cost of Care Study performed by Prudential Insurance Co.