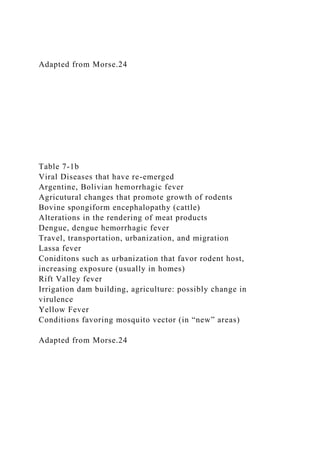
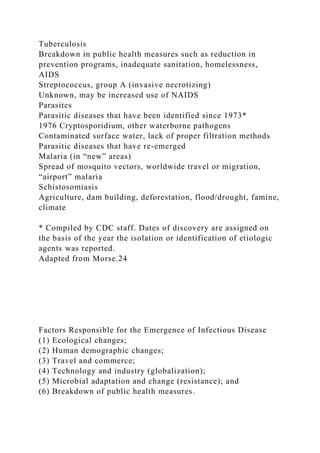
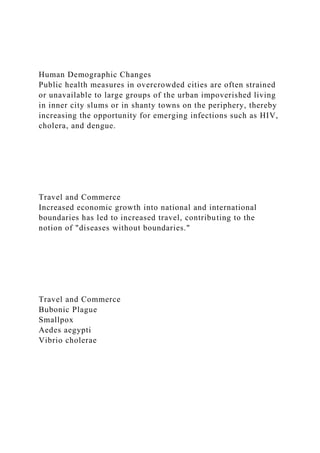
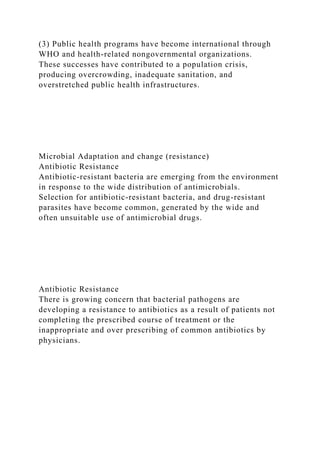
Chapter 7 of 'Living with the Earth' discusses emerging infectious diseases including Escherichia coli, AIDS, Ebola, and Hantavirus, emphasizing their global rise and factors contributing to their emergence. Key reasons for these diseases include ecological changes, human demographic shifts, travel, and globalization, which increase disease transmission and resistance. The chapter highlights the importance of understanding these diseases' epidemiology, characteristics, and practical approaches to limiting their spread.