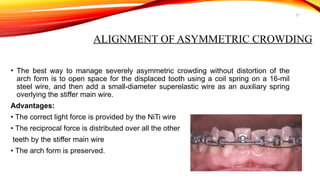
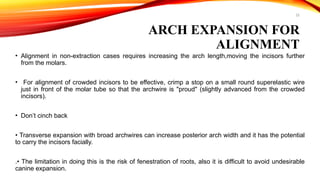
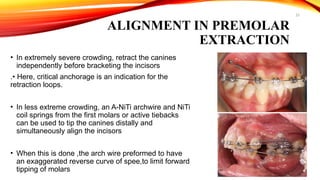
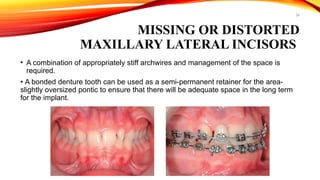
The document discusses the stages and objectives of orthodontic treatment, particularly focusing on the leveling and alignment phases to achieve proper dental occlusion. It details the principles, goals, and methods involved in aligning teeth, correcting malocclusions, and utilizing various archwire materials and designs. Additionally, it covers specific treatment approaches for crowding, crossbite correction, and the management of unerupted teeth.