Infectious Bursal Disease:Gumboro
Poultry Pathology(Path-611)
Lecture 8
Dr. Muhammad Kashif Saleemi
DVM PhD
Associate Professor (Tenured)
Member NDCC
Department of Pathology, Faculty of Veterinary Science,
University of Agriculture, Faisalabad, Pakistan
2.
Introduction and History
◼Infectious Bursal Disease (IBD) is an acute highly
contagious viral disease of young chicks having bursa of
Fabricius as primary target organ and immunosupression
◼ IBD was first reported in 1962 in Gumboro, Delware , USA
therefore disease is also named as Gumboro
◼ The immunosupressive role/effect of IBDV was first reported
by Allan in 1972
◼ IBD was controlled for many years with classical vaccines
prepared from early isolates
◼ In 1980 from Dalmarva USA variant serotype of IBD was
reported that is a persistent problem in Africa, Aisa, South
America, USA and Netherland (very virulent strain)
3.
The Town ofGumboro, Delaware in the United
States was the First Place where Gumboro
Disease was found in 1962.
4.
Etiology
◼ IBD iscaused by double stranded RNA virus belonging to
genus Avibirnavirus and family Birnaviridae
◼ The viral genome has two double stranded RNA segments
◼ The virus can be easily propagated in chicken embryos and
cell lines
◼ Two serotypes are present but serotype 1 is pathogenic
◼ Five viral proteins are present VP1, VP2, VP3, VP4 and VP5
◼ VP3 major protein is responsible for immunosupression
◼ VP2 is essential immunogen of IBDV
◼ VP1 protein is involved in virus replication process
◼ VP5 induced apoptosis in the infected cells by IBD virus
5.
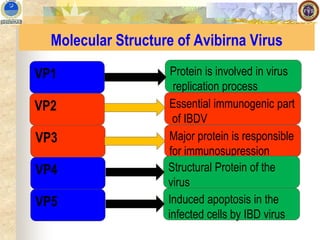
Molecular Structure ofAvibirna Virus
VP1
VP2
VP3
VP5
VP4
Protein is involved in virus
replication process
Essential immunogenic part
of IBDV
Major protein is responsible
for immunosupression
Structural Protein of the
virus
Induced apoptosis in the
infected cells by IBD virus
6.
Disinfection of Virusand Distribution of Disease
◼ This is a stable virus and is killed at pH 12 and no effect on
pH2
◼ This virus is very resistant to environmental factors and it
can survive for months in contaminated poultry houses and
for weeks in water, feed and droppings
◼ However it may be killed by formaldehyde and
glutaraldehyde and 0.05% NaOH
◼ Incidence with serotype 1 IBDV are worldwide in distribution
and present in all poultry producing areas of the world
◼ In Europe, Africa, Asia and South America vvIBD strains
predominate
7.
Natural Host andTransmission
◼ Chicken and turkey are natural host for IBDV, clinical disease
is most common in chicken however antibodies are present
in many free living birds
◼ Susceptible age for birds is 3-6 weeks.
◼ The virus is rapidly spreads through infected chicks,
contaminated premises and fomites to susceptible. The
disease is highly contagious
◼ No vertical transmission of IBD is reported
◼ The lesser meal worm harbors the virus for weeks after an
outbreak and may transmit virus to birds and it lives in poultry
litter
8.
Incubation Period andMortality
◼ Subclinical infections before 3 week age lead to destruction
of humoral immune response
◼ The virus is lymphocidal and severely damage the bursa of
Fabricius
◼ Immunosuppressive birds poorly respond to vaccines
◼ Incubation period is very short 2-3 days
◼ The passive immunization (MDA) is very important for the
prevention of early infection in birds (up to 2-3 weeks)
◼ Vaccination will be planned when MDA level is decreased
otherwise it will hinder proper working of vaccinal virus
◼ Morbidity is 100% and mortality 20-30 % but it may be
increased in vvIBDV strains
9.
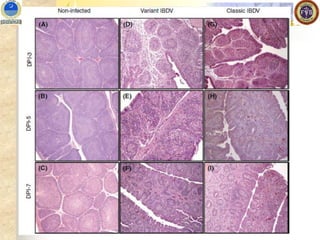
Pathogenesis
◼ Experimental reproductionof acute IBD in specific pathogen
free (SPF) white leghorn chickens, variant IBDV induce little if
any clinical signs and mortality but marked bursal lesions,
◼ Classical IBDV induces approximately 10%–50% mortality with
typical signs and lesions,
◼ vvIBDV induces approximately 50%–100% mortality with typical
signs and lesions .
◼ Detected histologic evidence of infection in the cloacal bursa
within 24 hours.
◼ In sequential studies of tissues from orally infected chickens
using immunofluorescence, viral antigen was detected in
macrophages and lymphoid cells in the cecum at 4 hours PI; a
hour later, virus was detected in lymphoid cells in the
duodenum and jejunum
10.
◼ The virusfirst reaches the liver, where it is detected 5
hours PI, It then enters the bloodstream, where it is
distributed to other tissues including the bursa; the bursal
infection is followed by a second massive viremia;
however, virus peak titer in the nonlymphoid organs is
several log10 lower than in the bursa and limited to the
viremic period.
◼ Studies of gene expression during acute IBD
demonstrated the activation of spleen macrophages and
of bursal T cells.
Pathogenesis
11.
Clinical Signs
◼ Clinicaldisease is observed only in birds after 3 weeks of
age and sudden onset of disease
◼ Depression, anorexia, ruffled feathers and drooping wings
◼ The chalky white diarrhea and dehydration and sometimes
voiding of blood and straining during defecation
◼ Vent picking is usually common and may be self inflicted
◼ The duration of clinical disease is one week and peak time
for mortality is 3-5 day of infection and gradually down
◼ IBD in white leghorn layers is more severe than broilers
◼ Increased clotting times in IBDV-infected chickens and
suggested that such coagulopathies could contribute to the
hemorrhagic lesions observed with this disease
12.
Gross Lesions
◼ Inacute phase bursa is swollen and inflamed with subserosal
edema and petechial to echymotic hemorrhages in the bursa
◼ Caseous exudate may be present in the bursal lumen due to
extensive necrosis and inflammation of bursal follicles in
acute phase of disease.
◼ The swelling recedes by 5th day and bursal atrophy is
completed within 8-10 days
◼ Day 3 bursa size start to increase and doubled at day 4 and
start to decrease at day 5 and atrophies at day 9-10 (1/3 of
normal size)
◼ At day 2-3 yellowish gelatinous material/transuadte will be
present in the cut surface of bursa
13.
Gross Lesions
◼ Increasedmucous in the intestine
◼ Petechial and echymotic hemorrhages are common on thigh
muscles, pectoral muscles
◼ Hemorrhages are also present at the junction of
proventriculus and gizzard
◼ The kidneys are swollen and urates may deposited in the
ureters leading to severe nephritis
◼ Atrophic and necrotic lesions may be present in other
lymphoid organs including thymus , cecal tonsils and payer
patches etc.
14.
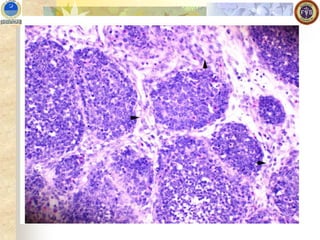
Microscopic Lesions
◼ Markedlymphoid follicles necrosis with heterophils rich
cellular infiltrates, edema and hyperemia followed by atrophy
and Interfollicular fibroplasia
◼ Starts at medullary region and soon lymphocytes are
replaced by heterophils, pyknotic debris, and hyperplasic
reticuloendothelial cells .
◼ All follicles are effected 3-4 days PI and inflammation
subsides cavities are developed in the medulla region
◼ Necrosis and phagocytosis of of plasma cells and hetrophils
◼ Initial depletion of T lymphocytes in first week followed by B
lymphocytes destruction and atrophies follicles indicate no B
cell
15.
Microscopic Lesions
◼ Transientlymphoid necrosis in spleen, thymus, payer
patches and Harderian glands
◼ Renal lesions are non specific with acute tubular necrosis,
casts of protein and some times heterophils
18.
Diagnosis and Control
◼Necropsy with signs and lesions
◼ Isolation and Identification
◼ Serological monitoring by ELISA most commonly used
◼ RT-PCR
◼ Differential Diagnosis from other related diseases like IBV.
Mycotoxicosis and CIA
◼ Proper immunization through good quality vaccines available
both live, and killed
◼ Live vaccines are classical, immune complex and Vector
vaccines
19.
Molecular Structure ofAvibirna Virus
VP1
VP2
VP3
VP5
VP4
Protein is involved in virus
replication process
Essential immunogenic part
of IBDV
Major protein is responsible
for immunosupression
Structural Protein of the
virus
Induced apoptosis in the
infected cells by IBD virus
20.
Diagnosis and Control
◼Biosecurity
◼ Use of Immune stimulants
◼ Diuretics to avoid kidney dammage
◼ Antipyretics and anti-inflammatory







































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)







