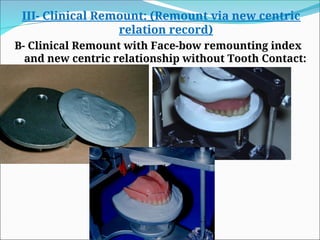
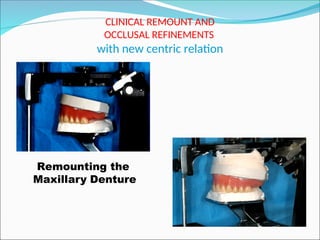
The document outlines the procedures and considerations for the insertion of complete dentures by Dr. Eman Husseiny Mohammed, focusing on the inspection of finished dentures, treatment during insertion, and post-insertion care. It details techniques for eliminating various errors in denture construction and occlusion, along with the importance of patient education regarding usage and chewing techniques with new dentures. Key aspects include ensuring proper fit, occlusal adjustments, and the need for personalized patient management to enhance adaptation to dentures.

![B-Treatment at the Time of Denture
Insertion
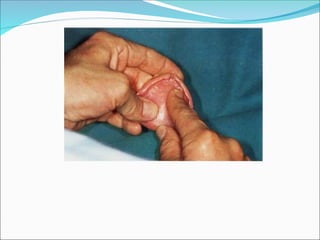
1) 1- Elimination of Basal Surface Errors [fitting
surface, Intaglio Surface]
any previous dentures out of the mouth for 12 to 24
hours immediately before the insertion appointment to
get the tissues healthy.
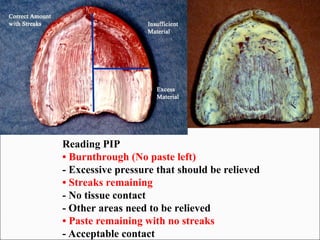
The use of pressure indicating paste is essential to
evaluate the accuracy of tissue contact especially when
- bilateral undercuts on residual ridge interfere with initial
placement of dentures
- When pressure spots are present or suspected in the final
impression.](https://image.slidesharecdn.com/lecturedentureinsertion-copy-241111064213-839c2684/85/lecture-denture-insertion-dif-Copy-ppt-6-320.jpg)