Stages of eczema
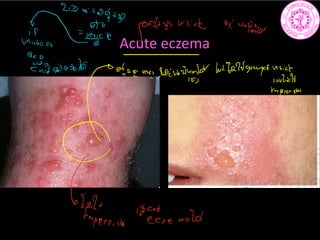
•Acute eczema: there is erythema, minute papules and
vesicles which may rupture leading to oosing and crust
formation.
• Subacute eczema: edema and vesiculation are less apparent
while papules, erythema and some scales are predominant
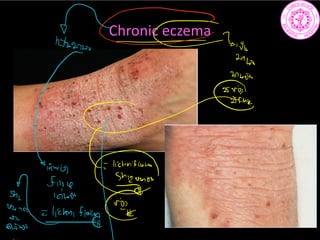
• Chronic eczema: no oosing or crusting are present. The skin
is dry, scaly and may be fissured. The repeated attacks of
pruritic skin may lead to lichenification which means:
thickening, hyperkeratosis, hyperpigmentation and
increased skin markings.
Into
iii
6st
sept 3sta
if
piiind089 ua cuetwb 17 c
stinarians 84 21 152 p athperpigment
ar
Enn
Cha
F
ftp.fifg
042m 052
84msec
Whperpigmatan a
crest
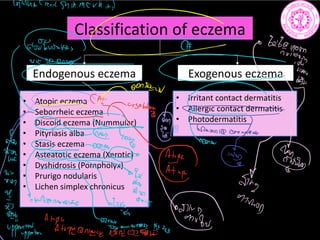
Classification of eczema
Endogenouseczema Exogenous eczema
• Atopic eczema
• Seborrheic eczema
• Discoid eczema (Nummular)
• Pityriasis alba
• Stasis eczema
• Asteatotic eczema (Xerotic)
• Dyshidrosis (Pompholyx)
• Prurigo nodularis
• Lichen simplex chronicus
• Irritant contact dermatitis
• Allergic contact dermatitis
• Photodermatitis
mm mm
i C
an
ii
tii l
figy
g
i
fgfgg.MIL
ii
Ji
Treatment of eczema
•Correction of underlying factors
Avoidance of exposure to sensitizers and solvents, treatment of varicose
veins, foci of infection, hot water etc.
• Broad spectrum antibiotics if secondary infection
• Oral antihistamines
• Topical corticosteroids of appropriate strength for the patient's age and
affected area twice daily for days. Creams are used for acute and
subacute cases and ointments for dry chronic cases
• Topical emollients as vaseline for dry skin and in chronic cases
• Topical immunomodulators: tacrolimus ointment 0.03% or pemicrolimus
1% cream twice daily
• Short course of systemic steroids in acute, severe and wide spread cases
• Ultraviolet rays therapy with PUVA and narrowband UVB (NBUVB)
a
mmesiit.tn
ii
irkatf
GE and in
322
steroid
26Jakewas
118mmol
be aging
if a band agg
unto
use
but if adamantasion ellulity iffunnair
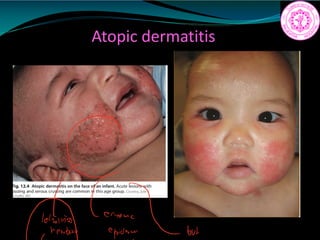
Atopic dermatitis
• 15–20%in early childhood
• Major features
- Pruritus
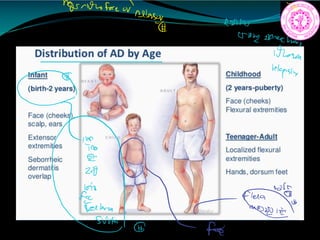
- Eczematous dermatitis (acute, subacute, or chronic) with
typical morphology and age specific patterns
Facial and extensor involvement in infancy
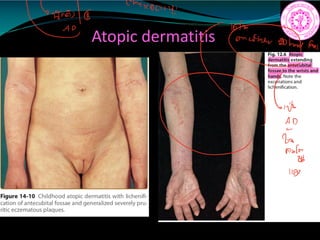
Flexural eczema/lichenification in children and adults
- Chronic or chronically relapsing disorder
- Personal or family history of atopy (allergic
rhinitis, asthma, atopic dermatitis)
2fleea
AP Ctropil
iffanis to animator
I80 maintain
childhood
a
CC
in infant 653 angina tidily
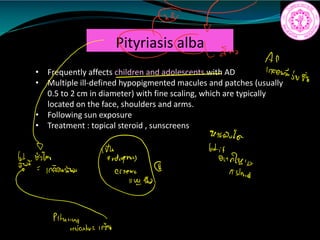
• Frequently affectschildren and adolescents with AD
• Multiple ill-defined hypopigmented macules and patches (usually
0.5 to 2 cm in diameter) with fine scaling, which are typically
located on the face, shoulders and arms.
• Following sun exposure
• Treatment : topical steroid , sunscreens
Pityriasis alba
Emo
AP
1500258
5N
96
ancestor
if g
Indus
Asteroid
Pitunyiu.vetoo
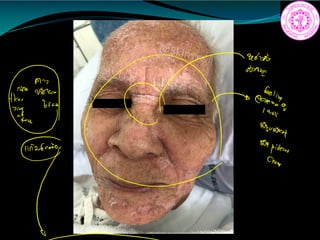
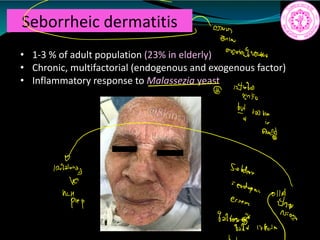
Seborrheic dermatitis
• 1-3% of adult population (23% in elderly)
• Chronic, multifactorial (endogenous and exogenous factor)
• Inflammatory response to Malassezia yeast
Ñ
2iwv
1
1
gang
10T
Solders
prep essen
iiii.IE
38.
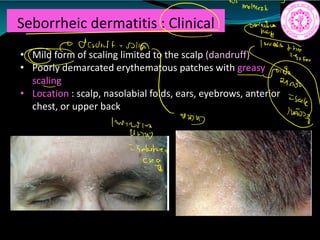
Seborrheic dermatitis :Clinical
• Mild form of scaling limited to the scalp (dandruff)
• Poorly demarcated erythematous patches with greasy
scaling
• Location : scalp, nasolabial folds, ears, eyebrows, anterior
chest, or upper back
malaise
a
dinner no
and
Invert is
Unu
Sebastien
Clegg
39.
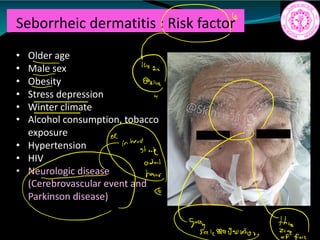
Seborrheic dermatitis :Risk factor
• Older age
• Male sex
• Obesity
• Stress depression
• Winter climate
• Alcohol consumption, tobacco
exposure
• Hypertension
• HIV
• Neurologic disease
(Cerebrovascular event and
Parkinson disease)
r
H
aaw
th
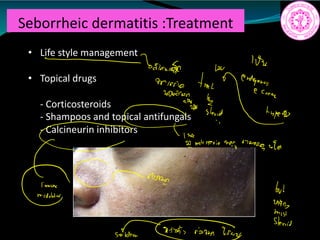
Seborrheic dermatitis :Treatment
•Life style management
• Topical drugs
- Corticosteroids
- Shampoos and topical antifungals
- Calcineurin inhibitors
in
a
tritt that
on
To
sled ea
1
molasserio
wey anionrota
Crm but
I
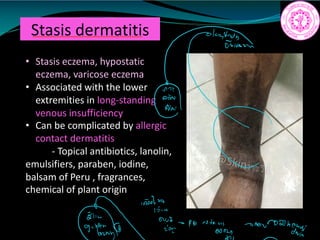
Stasis dermatitis
• Stasiseczema, hypostatic
eczema, varicose eczema
• Associated with the lower
extremities in long-standing
venous insufficiency
• Can be complicated by allergic
contact dermatitis
- Topical antibiotics, lanolin,
emulsifiers, paraben, iodine,
balsam of Peru , fragrances,
chemical of plant origin
an
retiring among
44.
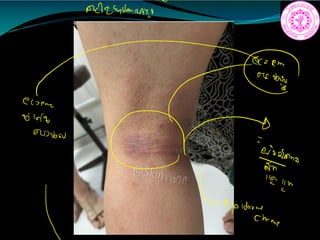
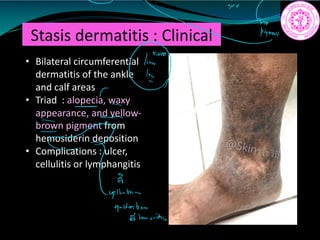
Stasis dermatitis :Clinical
• Bilateral circumferential
dermatitis of the ankle
and calf areas
• Triad : alopecia, waxy
appearance, and yellow-
brown pigment from
hemosiderin deposition
• Complications : ulcer,
cellulitis or lymphangitis
IGma
a
8
yellenbrin
a denftenaid.mn
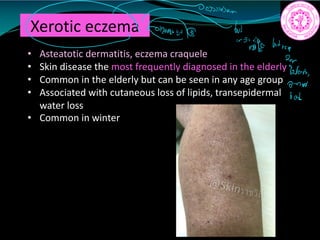
Xerotic eczema
• Asteatoticdermatitis, eczema craquele
• Skin disease the most frequently diagnosed in the elderly
• Common in the elderly but can be seen in any age group
• Associated with cutaneous loss of lipids, transepidermal
water loss
• Common in winter
in
inside btrare
2
Wow
0771N
bob
48.
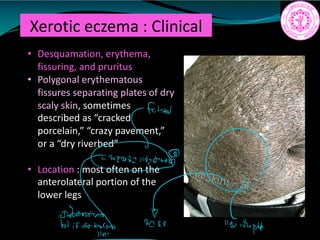
Xerotic eczema :Clinical
• Desquamation, erythema,
fissuring, and pruritus
• Polygonal erythematous
fissures separating plates of dry
scaly skin, sometimes
described as “cracked
porcelain,” “crazy pavement,”
or a “dry riverbed”
• Location : most often on the
anterolateral portion of the
lower legs
fation
f1t .tk
i i adult
49.
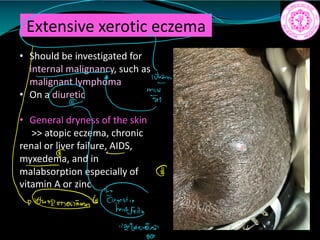
Extensive xerotic eczema
•Should be investigated for
internal malignancy, such as
malignant lymphoma
• On a diuretic
• General dryness of the skin
>> atopic eczema, chronic
renal or liver failure, AIDS,
myxedema, and in
malabsorption especially of
vitamin A or zinc
C
pantsuit
11
295
0552
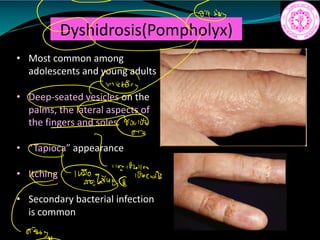
Dyshidrosis(Pompholyx)
• Most commonamong
adolescents and young adults
• Deep-seated vesicles on the
palms, the lateral aspects of
the fingers and soles
• “Tapioca” appearance
• Itching
• Secondary bacterial infection
is common
0tG
91 no
85502
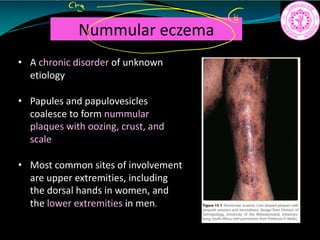
Nummular eczema
• Achronic disorder of unknown
etiology
• Papules and papulovesicles
coalesce to form nummular
plaques with oozing, crust, and
scale
• Most common sites of involvement
are upper extremities, including
the dorsal hands in women, and
the lower extremities in men.
I
crine
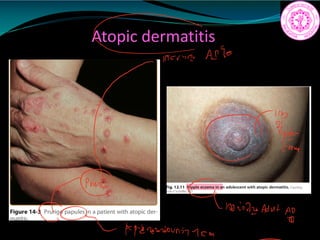
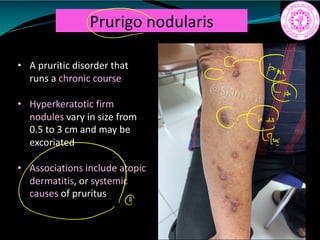
Prurigo nodularis
• Apruritic disorder that
runs a chronic course
• Hyperkeratotic firm
nodules vary in size from
0.5 to 3 cm and may be
excoriated
• Associations include atopic
dermatitis, or systemic
causes of pruritus
c
ftp.G
C
Lan
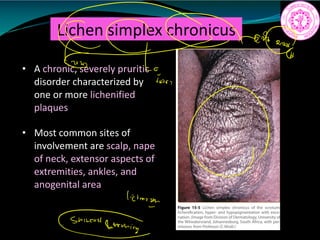
Lichen simplex chronicus
•A chronic, severely pruritic
disorder characterized by
one or more lichenified
plaques
• Most common sites of
involvement are scalp, nape
of neck, extensor aspects of
extremities, ankles, and
anogenital area
lictimist
Shinchstemoning
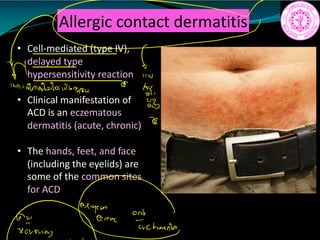
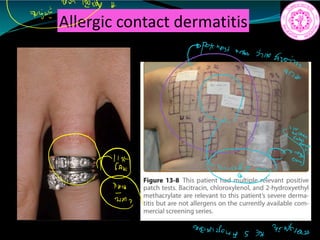
Allergic contact dermatitis
•Cell-mediated (type IV),
delayed type
hypersensitivity reaction
• Clinical manifestation of
ACD is an eczematous
dermatitis (acute, chronic)
• The hands, feet, and face
(including the eyelids) are
some of the common sites
for ACD
M 11W
inardaladalaithner
y
i
ñ
Fiurio
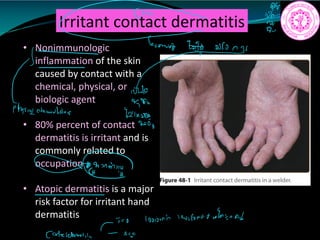
Irritant contact dermatitis
•Nonimmunologic
inflammation of the skin
caused by contact with a
chemical, physical, or
biologic agent
• 80% percent of contact
dermatitis is irritant and is
commonly related to
occupation
• Atopic dermatitis is a major
risk factor for irritant hand
dermatitis
N
Yift
1 Who
470
ptysigatomialla.us
8211429
p
GerminG
looioni twifordtwfai.sn
Cotcldematii I
63.
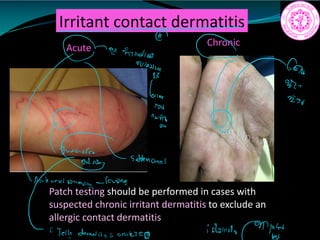
Irritant contact dermatitis
Acute
Patchtesting should be performed in cases with
suspected chronic irritant dermatitis to exclude an
allergic contact dermatitis
Chronic
a
feminine
ms
Vinny 002
6110
row
i
suddennial
Elina
oppitch
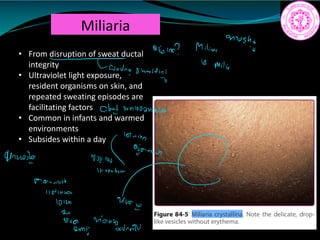
Miliaria
• From disruptionof sweat ductal
integrity
• Ultraviolet light exposure,
resident organisms on skin, and
repeated sweating episodes are
facilitating factors
• Common in infants and warmed
environments
• Subsides within a day
moshi
dearie Milian
US
Milio
Tone sweatdish
Cloud
wnlooonnio m.ie
Tourisick
lifinson
101m 400
2
aug monsoon
nN
2mi
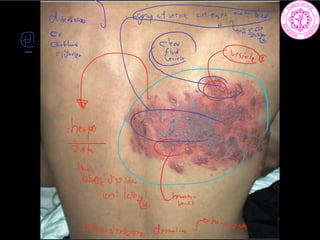
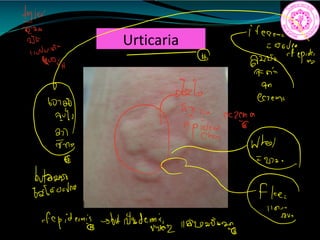
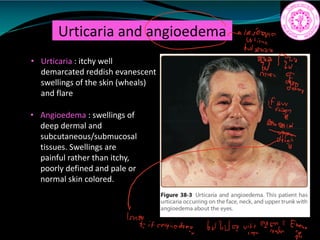
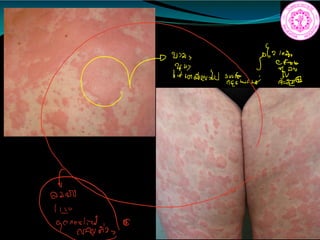
Urticaria and angioedema
•Urticaria : itchy well
demarcated reddish evanescent
swellings of the skin (wheals)
and flare
• Angioedema : swellings of
deep dermal and
subcutaneous/submucosal
tissues. Swellings are
painful rather than itchy,
poorly defined and pale or
normal skin colored.
flavono
It'sb
200 Pro
Inn
Fem
IEY.EE
881
11
n
if angioedema
butbvavityettaifh.gs
71.
Urticaria : pathophysiology
•Allergic : histamine is an important mediator in urticaria. Mast
cells are the major histamine releasing cells in the skin.
Allergens react with IgE molecules which are bound to the
surface of mast cells leading to mast cell degranulation and
release of histamine and other mediators. This results in local
increase of permeability of capillaries and venules.
• Non allergic : direct degranulation of mast cells occurs without
antigen antibody reaction due to the effect of substances like
- aspirin, neuropeptides, nonsteroidal anti-inflammatory
drugs (NSAID), opiates, ciprofloxacin, polymixin, rifampicin and
vancomycin
we Unreamestrellor histamine
4128841022
Tomiskell
Efs
Gouldroscions
has
i.ie
i
i
10220
trainman mistreat
2 pathing
72.
Causes of urticaria
1-Food: food additives or preservatives, fishes, banana, nuts, eggs,
chocolate and cheese.
2- Drugs: aspirin, NSAIDs, antibiotics eg; penicillin..etc
3- Inhalants: pollens, dust or animal fur
4- Intestinal parasites
5- Stress
6- Septic foci eg; in teeth, tonsils or urinary tract
7- Physical causes: heat, cold, water, vibration, sunlight or pressure
8- Cholinergic urticaria: is a specific type in which small weals occur
in association with sweating due to heat or emotional stress
9- Insect bites or stings
10- Contact urticaria eg; occupational exposure
11- Medical causes: like hepattitis, obstructive jaundice and
Helicobacter pylori infection
12- Serum sickness
I
analata
PUawidaiauiwonvessoo.tl02TUiwodr
worse a
É
in
fdt
panwodamide
provaana
ita arrannigtiitiFet
27109 onnankiaci.us
73.
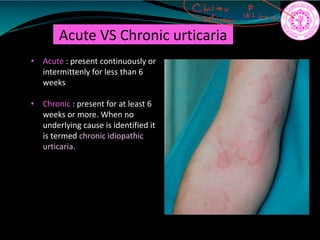
Acute VS Chronicurticaria
• Acute : present continuously or
intermittenly for less than 6
weeks
• Chronic : present for at least 6
weeks or more. When no
underlying cause is identified it
is termed chronic idiopathic
urticaria.
cai wt
74.
Urticaria: treatment
1-Treatment ofthe cause if possible
2- AntiH1 antihistamines are the first line of treatment:
- traditional classic antiH1 eg; chlorpheneramine maleate,
diphenhydramine, and hydroxizine
- non sedating antiH1: cetrizine hydrochloride, loratadine,
fexofenadine, desloratadine and acrivastine
3- AntiH2 antihistamines may be needed in addition to antiH1 eg;
cimetidine and ranitidine
4- Systemic drug
5- Locally: calamine lotion is used for soothing the sensation of
pruritus.
6- In angioedema: distressing the respiratory passages from
oropharyngeal-laryngeal edema; epinephrine (adrenaline) in 1/1000
solution is the first line of management. It is given subcutaneously in
a dose ml. -
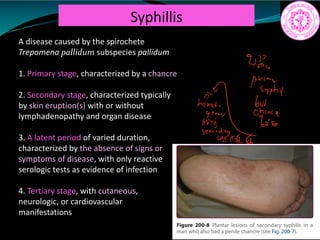
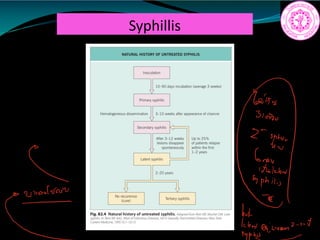
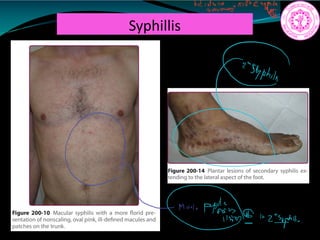
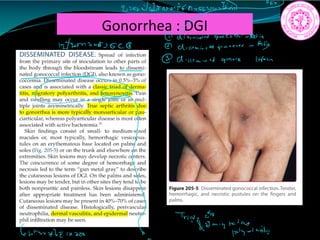
Syphillis
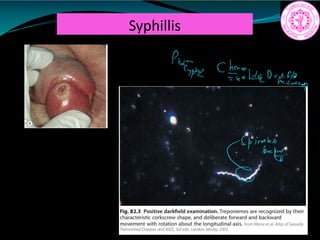
A disease causedby the spirochete
Trepomena pallidum subspecies pallidum
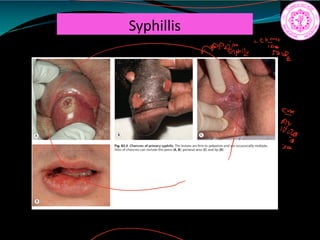
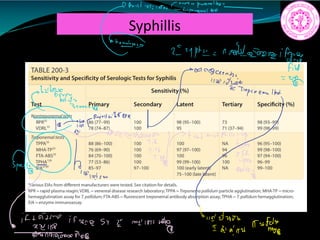
1. Primary stage, characterized by a chancre
2. Secondary stage, characterized typically
by skin eruption(s) with or without
lymphadenopathy and organ disease
3. A latent period of varied duration,
characterized by the absence of signs or
symptoms of disease, with only reactive
serologic tests as evidence of infection
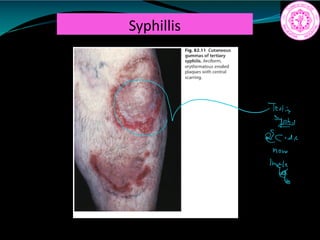
4. Tertiary stage, with cutaneous,
neurologic, or cardiovascular
manifestations
prime
syphil
Iis
Secondary Syphillis
Prodomal symptoms
Generalizedlymphadenopathy (50-85%)
Skin manifestatons
- Early (10%): generalized eruption; non-pruritic, roseola-like,
discrete macules
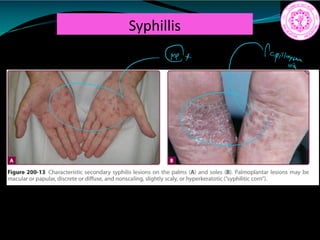
- Late (70%): generalized maculopapular and papulosquamous
eruptions
– Palms and soles: symmetric papules and plaques with a collarette
of scale (Biett collaretes)
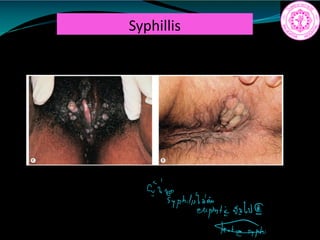
– Anogenital area: condyloma lata
– Seborrheic area: “corona veneris” along the hairline
Mucous membrane (30%)
- Mucous patches
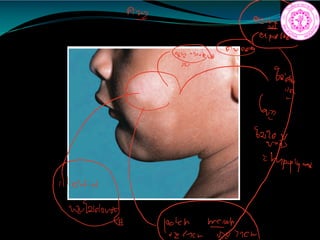
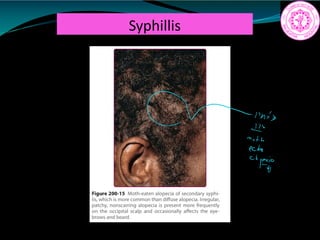
Patchy alopecia (7%) “moth-eaten” localized areas of hair loss
c Try
so mean a batwar 6
note
it
202
c Ic
t.tn iwyTtge
Sous
14200
Morph in
mi c
iiiii an
iffaint
pole s le
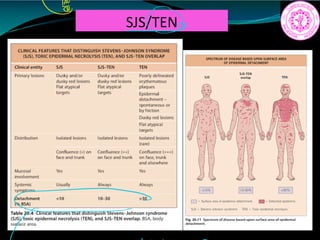
Stevens-Johnson syndrome/toxic epidermal
necrolysis(SJS/TEN)
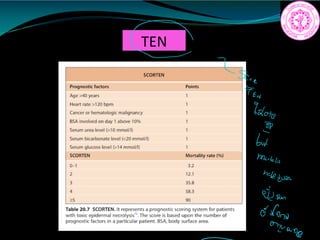
- Mortality rate for SJS 1- 5 %, TEN 25–35 %
- Variants of epidermal necrolysis
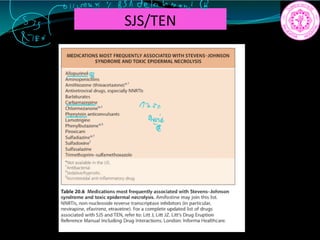
- They occur 4–28 days after drug exposure
- Mycoplasma pneumoniae, Herpes simplex virus was recognized in
several cases of SJS, especially in children
- Factors that seem to impact on the incidence of SJS and TEN: the
genetic background of patients (HLA, metabolizing enzymes), the
coexistence of cancer, concomitant radiotherapy, and certain infectious
diseases (e.g., HIV)
Lancet,Vol 390 October 28, 2017
4T
off death
mag
egg
ale amazing bairnsamidst
fEugnm.gg
epidermenecrolies
qt
da.lu
epidemtnEt ifeaemeepidermislaio
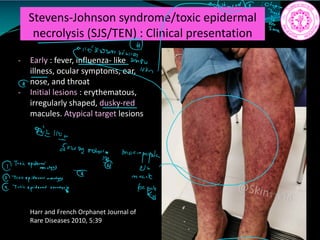
120.
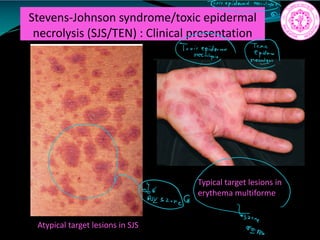
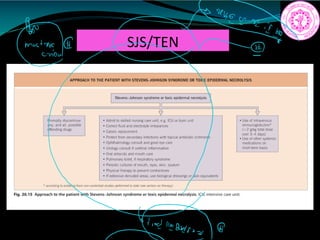
Stevens-Johnson syndrome/toxic epidermal
necrolysis(SJS/TEN) : Clinical presentation
- Early : fever, influenza- like
illness, ocular symptoms, ear,
nose, and throat
- Initial lesions : erythematous,
irregularly shaped, dusky-red
macules. Atypical target lesions
Harr and French Orphanet Journal of
Rare Diseases 2010, 5:39
Iii
right
money.name mppI
Tonicepiderminy
Cb
mail
it t.ie
121.
Stevens-Johnson syndrome/toxic epidermal
necrolysis(SJS/TEN) : Clinical presentation
Atypical target lesions in SJS
Typical target lesions in
erythema multiforme
Trxicepidermalnav.lyg
TriaieGEEIa. h
a
ne
Elow
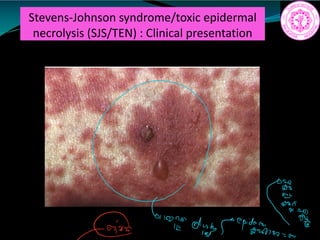
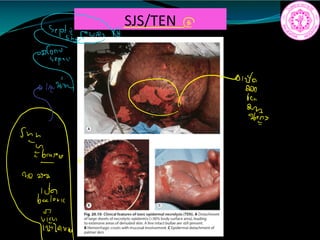
Stevens-Johnson syndrome/toxic epidermal
necrolysis(SJS/TEN) : Clinical presentation
- Necrotic lesion confluence leads to
extensive erythema, flaccid
blisters, and large epidermal
sheets
- Nikolsky sign
m
brinating
into
124.
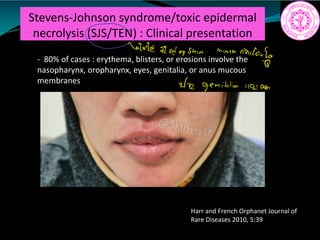
Stevens-Johnson syndrome/toxic epidermal
necrolysis(SJS/TEN) : Clinical presentation
- 80% of cases : erythema, blisters, or erosions involve the
nasopharynx, oropharynx, eyes, genitalia, or anus mucous
membranes
Harr and French Orphanet Journal of
Rare Diseases 2010, 5:39
1
Gate and a shin mussa
rindouf
In genitalia 1101non
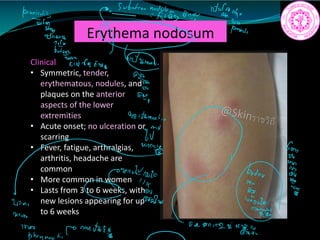
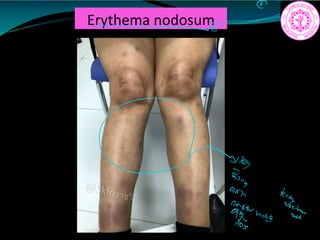
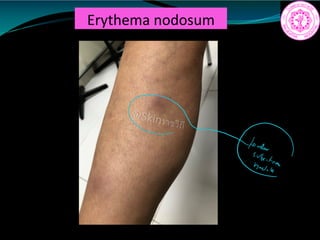
Erythema nodosum
Clinical
• Symmetric,tender,
erythematous, nodules, and
plaques on the anterior
aspects of the lower
extremities
• Acute onset; no ulceration or
scarring
• Fever, fatigue, arthralgias,
arthritis, headache are
common
• More common in women
• Lasts from 3 to 6 weeks, with
new lesions appearing for up
to 6 weeks
tanniality
gs't.to
Easontw
hy
g
Byan
yyppy.name
I
EI
µ
W
una
iii
win rain
Union
EA
8111214844
phanngiti.TMUE.nl
135.
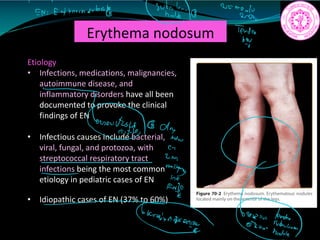
Erythema nodosum
Etiology
• Infections,medications, malignancies,
autoimmune disease, and
inflammatory disorders have all been
documented to provoke the clinical
findings of EN
• Infectious causes include bacterial,
viral, fungal, and protozoa, with
streptococcal respiratory tract
infections being the most common
etiology in pediatric cases of EN
• Idiopathic cases of EN (37% to 60%)
1 7 91
EN Eutheranoulestly
g 2kg
Te
draw
Eis
T.name ii.t