The document discusses various periradicular lesions of pulpal origin, including:
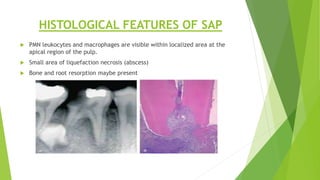
1) Symptomatic apical periodontitis, which presents with pain and responsive tests and may be associated with radiolucency; histologically there is PMN infiltration and bone/root resorption.
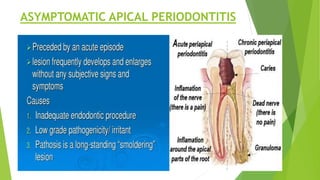
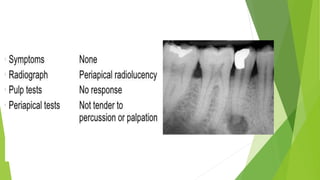
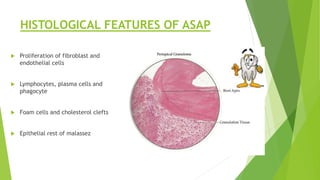
2) Asymptomatic apical periodontitis, seen radiographically as fibroblast and inflammatory cell proliferation without pain.
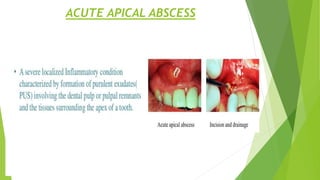
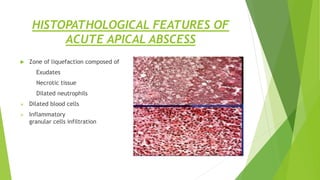
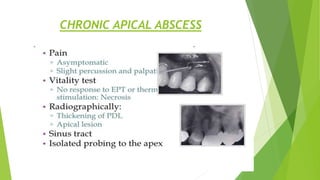
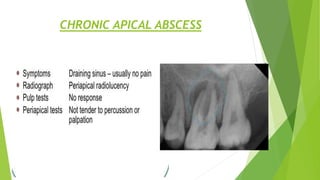
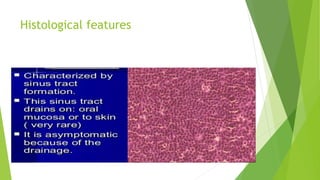
3) Acute/chronic apical abscess, presenting clinically as swelling and histologically as zones of necrosis infiltrated by neutrophils and inflammatory cells.