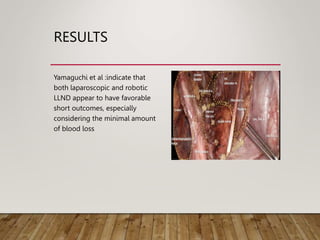
This document summarizes recent literature on lateral lymph node dissection (LLND) in rectal cancer surgery. LLND aims to reduce the risk of lateral local recurrences, which can occur when lateral lymph nodes are metastatic. The literature discusses indications for and techniques of LLND. Prophylactic LLND may increase complications while selective LLND for suspicious lymph nodes above 7mm may decrease local recurrences. LLND can be performed laparoscopically or robotically with favorable short-term outcomes compared to open surgery, though it carries risks of morbidity. Definitions of suspicious lymph nodes vary between studies.