Download to read offline









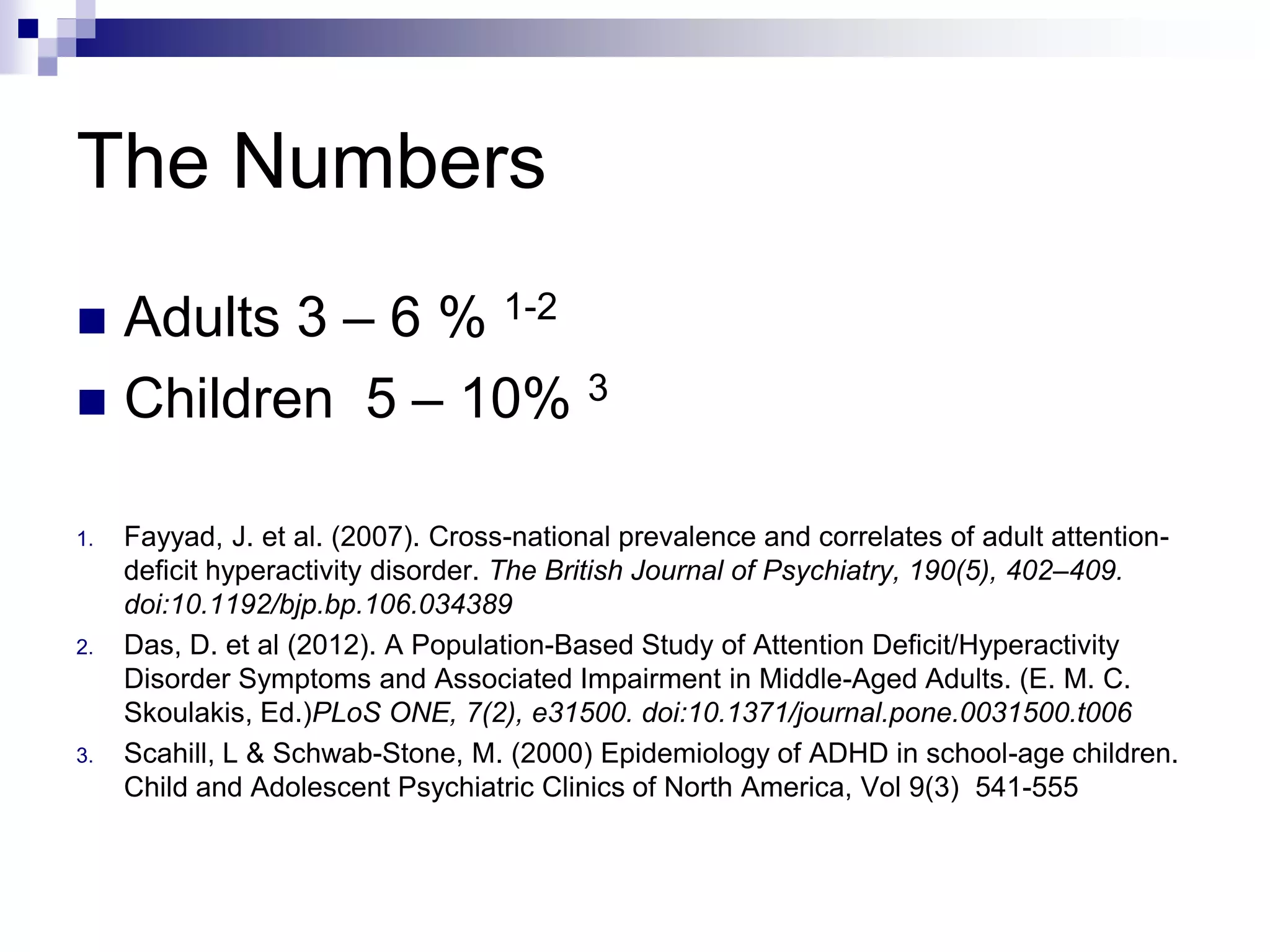










The presentation by Dr. Mahendra Perera discusses adult ADHD as both a clinical reality and the importance of accurate diagnosis and management. It highlights the prevalence of ADHD, its core symptoms, co-morbidities, and emphasizes a bio-behavioral approach to treatment, which includes illness education, behavioral modification, and medication options. The conclusion underscores ADHD as a lifetime condition requiring ongoing medical attention and a multimodal approach to support patients effectively.