1. The effects of topical icing after contusion injury on angiogenesis in regenerating skeletal muscle
Jonathan Peake1, Daniel Singh1, Zohreh Barani Lonbani1, Mia Woodruff1, Tony Parker1, Roland Steck1,2
1Tissue Repair and Regeneration Group; Institute of Health and Biomedical Innovation; 2Medical
Engineering Research Facility; Queensland University of Technology, Brisbane, Australia
ABSTRACT (Program no. 862.5) We investigated the effects of topical icing after muscle contusion injury on angiogenesis in regenerating skeletal muscle. Male Wistar rats
were subjected to contusion injury by dropping a cylindrical-shaped weight (370 g) on the biceps femoris muscle of one leg. Within 5 min after injury, a block of ice
(contained within a paper cup) was applied to the skin surrounding the muscle for 20 min. Control groups received no ice treatment. The rats were euthanized at 1, 3, 7
and 28 days post-injury (n=24 per time point). In 12 rats in each group, a punch biopsy (diameter: 8 mm) was taken from the region of injury and fixed in 10% neutral
buffered formalin. Tissue sections (5 m) were then mounted on glass slides for immunohistochemical analysis of CD68+ macrophages, vascular endothelial growth factor
(VEGF) and von Willebrand’s factor (vWF). After euthanasia, the others rats in each group were flushed with heparinised saline, and then perfused with a radio-opaque
contrast agent using an infusion pump. Muscle biopsies were also collected from these rats, and analyzed to determine blood vessel volume and number using high
resolution micro computed tomography (CT). Macrophage numbers were lower at all time points, VEGF expression was lower at 3 days, while vWF expression was at 3
and 7 days post-injury in the icing group versus the non-icing group (p<0.05). By contrast, VEGF expression was higher at 28 days post-injury in the icing group versus the
non-icing group (p<0.05). Muscle fibre cross-sectional area was not significantly different between the groups at 7 or 28 days post-injury. The proportion of regenerating
muscle fibres was also not significantly different between the groups at 7 days post-injury, whereas it was higher at 28 days in the icing vs non-icing group (p<0.05).
Although the muscle vasculature could be visualised using micro CT, changes in vessel number and volume were variable, and there were no significant group differences.
In conclusion, topical icing suppressed inflammation and delayed angiogenesis in regenerating muscle. However, these responses did not affect muscle regeneration.
Background
Cryotherapy in the form of icing and immersion in ice baths has traditionally been used to treat soft tissue injuries. The rationale for using these treatments
centres around providing pain relief, reducing tissue metabolism, and altering vascular responses to minimise oedema. By reducing the metabolic rate of
tissues within and around the injury site, cryotherapy may protect the healthy bystander cells from the ischemic environment in the immediate period after
injury, thereby reducing the risk of secondary cell injury or death. Some experimental evidence exists to support this concept1,2. Other research has also
demonstrated that cryotherapy reduces leukocyte adhesion and rolling, neutrophil infiltration and activation, and production of reactive oxygen species in
muscle following injury3,4,5,6. However, another more recent study reported that topical icing of muscle after crush injury delayed macrophage infiltration,
attenuated the IGF-1 expression and satellite cell activity, caused greater fibrosis and impaired muscle growth7. Despite the importance of angiogenesis in
tissue regeneration, no research has investigated the effects of cryotherapy on angiogenesis following muscle injury. Therefore, the aim of this study was to
examine how cryotherapy affects angiogenesis in the days and weeks after muscle contusion injury.
Methods
• Eighty adult male Wistar rats were used for this study. They were divided into icing and non-icing groups
(n=40 per group).
• The rats were anaesthetised by isofluorane inhalation before they were placed on a device to induce muscle.
• A muscle contusion injury was induced using a custom-made rig (Figure 1).
• The right hindlimb was placed in an extended position on a platform in which a flat-bottomed, cylindrical
370-g weight was dropped from a height of 1.66 m. The left limb served as non-injured control.
• The weight was positioned specifically to impact the biceps femoris muscle to cause a substantial skeletal
muscle injury without perforating the skin or causing bone fracture.
• Five minutes after the contusion injury was induced, an ice block was applied to the skin surrounding the
injured muscle for 20 min. A 5-cm diameter cylindrical ice block, set in a paper cup, was massaged in a figure
8 motion on the injured area without compression. Icing was performed while the rats were anaesthetised.
• A 50-ml flat-bottomed beaker (maintained at room temperature) was used to massage the injured area of
the non-icing group, to simulate the application and pressure of the ice blocks.
• The rats were euthanised by CO2 asphyxiation at 1, 3, 7 and 28 days after injury. A sub-group of 32 rats was
flushed with heparinised saline, and then perfused with a radio-opaque contrast agent (Microfil, MV 122,
Flowtech, USA) using an infusion pump (Figure 3). After the contrast agent was perfused, the damaged and
non-injured control legs were removed.
• In all rats, an 8-mm muscle biopsy was taken from the region of interest in both the injured and control legs.
Muscle biopsies for 32 rats were analyzed to determine blood vessel volume and number using high
resolution micro computed tomography (CT). Muscle biopsies from the other 48 rats were fixed in 10%
Figure 1: Illustration and photo of
custom-made contusion injury device
Figure 2: Experimental procedure to
perfuse radio-opaque contrast agent
neutral buffered formalin for one day, dehydrated through a serial ethanol series, processed and then embedded in paraffin wax.
• The cylindrical biopsy samples were transversely orientated during embedding to ensure sections were cut from the region of interest. Transverse serial
sections 5-µm thick were cut using a microtome and mounted on poly-L-lysine adhesion glass slides. Sections between 50 µm and 250 µm below the biopsy
surface were used for analysis.
• Slides were stained with haematoxylin and eosin for qualitative histological analysis of muscle damage and regeneration, mouse monoclonal anti-CD68
(ED1) antibody (1:200 dilution; Abcam, Cambridge, USA) to identify macrophages, rabbit polyclonal anti-human von Willebrand’s factor (Ready-to-use;
DAKO, California, USA) to identify endothelial cells (capillaries) and rabbit polyclonal anti-human vascular endothelial growth factor A-20 (sc-152, 1:200;
Santa Cruz Biotechnology, Santa Cruz, USA).
• Colour was developed using 3,3-diaminobenzidine (DAB substrate kit; DAKO, California, USA) followed by counter stain with Mayer’s haematoxylin.
• Slides were viewed using light microscopy and images were captured using the Zeiss Axio Zen 2011 image analysis software. Using 40 magnification, 10
fields of view were captured and quantified for each sample. Image J software was used to quantify areas of positive staining.
• Cross-sectional area of muscle fibres was assessed by tracing the outline of X fibres, and using software to calculate the fibre area. Regenerating fibres were
identified as those fibres with centrally located nuclei and expressed as a proportion of the total number of fibres in X fields.
• Data were analysed using 2 factor repeated measures ANOVA and unpaired t tests
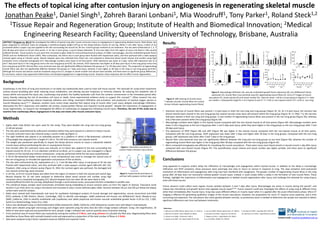
Results
• Extensive necrosis of muscle fibres was present 1 d post-injury in both the non-icing and icing groups (Figure 3C, D). At 3 d post-injury, the necrosis had
almost entirely been cleared in the non-icing group but several necrotic areas were still present within the icing group (Figure 3E, F). After 7 d, the necrosis
had been cleared in both non-icing and icing groups. A vast number of regenerating muscle fibres was present in the non-icing group (Figure 3G), whereas
only a few were present within the icing group (Figure 3H).
• Macrophage numbers were higher in the injured muscle compared with the non-injured muscle at all time points (Figure 4A). Macrophage numbers were
lower in the icing group vs the non-icing group after 1 and 3 days post-injury, while they were higher in the icing groups vs the non-icing groups after 7 and
28 days post-injury.
• The expression of VEGF (Figure 4B) and vWF (Figure 4B) was higher in the injured muscle compared with the non-injured muscle at all time points.
Compared with the non-icing groups, VEGF expression was lower after 3 days and higher after 28 days in the icing groups. Compared with the non-icing
groups, vWF expression was lower after 3 and 7 days in the icing groups.
• Muscle fibre cross-sectional area was not significantly different between the icing and non-icing groups at any time (Figure 4D), whereas the number of
regenerating muscle fibres was higher in the icing group after 28 days compared with the non-icing groups (Figure 4E)
• Micro computed tomography was effective for visualising the muscle vasculature. There were many more blood vessels in injured muscle 1 day after injury
compared with non-injured muscle (Figure 4F). The quantification vessel volume and vessel number was highly variable, and there were no significant
differences between the groups.
Figure 3: H&E staining of muscle tissue.
* indicates necrotic muscle fibres (no nuclei).
Arrows indicate regenerating muscle fibres).
Icing
Non-icing
Non-injured Injured
F
Figure 4: Macrophage infiltration (A), vascular endothelial growth factor expression (B), von Willebrand’s factor
expression (C), muscle fibre cross-sectional area (D), regenerating muscle fibres (E), micro-CT images of muscle
vasculature (F), vessel volume (G) and vessel number (H). Data are mean SD for n=6 per group in Figures AE. Data
are median interquartile range for n=4 in Figures G and H.* P < 0.05 vs non-injured control. # P < 0.05 vs non-icing.
Conclusions
Icing appeared to suppress and/or delay the infiltration of macrophages and angiogenesis within injured muscle. In addition to the delay in macrophage
infiltration and VEGF activation, these processes were seemingly also slow to return to normal in response to icing. The slow activation (and protracted
resolution) of inflammation and angiogenesis after icing may have interfered with myogenesis. The greater number of regenerating muscle fibres in the icing
group after 28 days does not necessarily indicate greater muscle repair. Instead, it could simply reflect a delay in the formation of new muscle fibres. These
findings highlight the importance of inflammation and angiogenesis in skeletal muscle regeneration after injury, and challenge the rationale for using icing to
treat soft tissue injuries.
Future research could collect more regular muscle samples between 3 and 7 days after injury. Macrophages are active in muscle during this period7, and
release key chemokines and growth factors that regulate muscle repair8,9,10. Future research could also investigate the effects of using icing at different times
other than immediately after muscle injury. Icing may cause different effects on muscle repair when it is applied after the acute inflammatory phase. Micro CT
imaging is effective for generating qualitative images of the muscle vasculature. However, the preparation for micro CT requires some expertise, and is time
consuming and expensive. The vasculature also varies greatly between animals, so preliminary work is needed to determine the sample size required to detect
significant differences over time and between treatments.
References
1. Merrick et al 1999. Med Sci Sports Exerc 31: 1516-21 5. Lee et al 2005. Med Sci Sports Exerc 37: 1093-8 9. Arnold et al 2007. J Exp Med 204: 1057-69
2. Merrick et al 2010. J Sport Rehabil 19: 380-8 6. Carvalho et al 2010. J Sports Sci 28: 923-35 10. Hammers et al 2015. J Appl Physiol (in press)
3. Schaser et al 2006. J Trauma 61: 642-9 7. Takagi et al 2011. J Appl Physiol 110: 382-8
4. Schaser et al 2007. Am J Sports Med 35: 93-102 8. Lu et al 2001. FASEB J 25: 358-69
Contact email: jonathan.peake@qut.edu.au