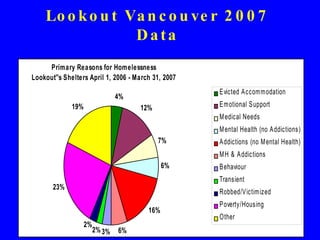
The document discusses homelessness and health in Canada. It provides an overview of Dr. James Frankish's research interests related to homelessness, poverty, and marginalized groups. It summarizes data on the characteristics of homeless populations in Vancouver and BC, including health issues, reasons for homelessness, and needed services. It also discusses strategies for addressing homelessness, including changing public discourse, using housing to facilitate intersectoral collaboration, and specific housing and support policies.


































![Contact Information Dr. Jim Frankish, Senior Scholar, Michael Smith Foundation Director, Centre for Population Health Promotion Research Rm 425, Library Processing Centre 2206 East Mall Vancouver BC V6T 1Z3 604-822-9205, 822-9210, [email_address] Personal Website: jimfrankish.com Partners in Community Health Research www.pchr.net](https://image.slidesharecdn.com/jims-homelessness-presentation-1200859210372991-5/85/Jim-s-Homelessness-Presentation-37-320.jpg)

































![Social issues[1]](https://cdn.slidesharecdn.com/ss_thumbnails/socialissues1-100623115123-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Social issues[1]](https://cdn.slidesharecdn.com/ss_thumbnails/socialissues1-100623140014-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































