هذا الملف يحتوي على المحاضرة الأولى في مادة التركيبات المتحركة الجزئية (Removable Partial Prosthodontics). الهدف من رفعه هو مراجعة المحتوى، وفهم المفاهيم الرئيسية، وتحضير أسئلة للمذاكرة والاستعداد للامتحان
INTRODUCTION TO REMOVABLE
PARTIALPROSTHODONTICS
faculty of dentistry
department of prosthodontics
Dr. Mais M Odah Dr. Mahmoud Hasasna PhD IN Prosthodontics
BDS, MClinDent in Prosthodontics
Palestinian Board
2.
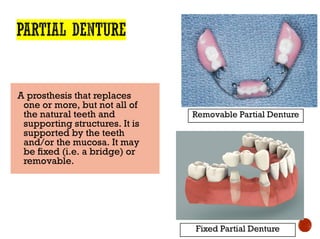
A prosthesis thatreplaces
one or more, but not all of
the natural teeth and
supporting structures. It is
supported by the teeth
and/or the mucosa. It may
be fixed (i.e. a bridge) or
removable.
Removable Partial Denture
Fixed Partial Denture
3.
Loading…
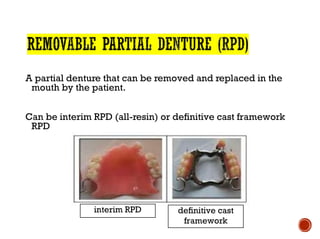
A partial denturethat can be removed and replaced in the
mouth by the patient.
Can be interim RPD (all-resin) or definitive cast framework
RPD
interim RPD definitive cast
framework
4.
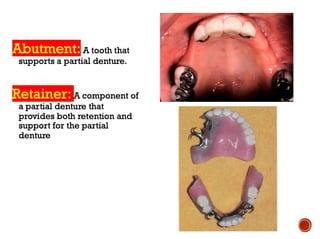
A denture used
fora short
interval of time
to provide:
a. esthetics, mastication,
occlusal support and
convenience.
b. conditioning of the
patient to accept the final
prosthesis.
5.
Loading…
Retention:
Resistance to removalfrom the tissues or teeth
Stability:
Resistance to movement in a horizontal direction (anterior-
posteriorly or medio-laterally)
Support:
Resistance to movement towards the tissues or teeth
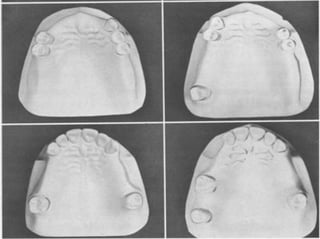
· should permitimmediate visualization of the type of
partially edentulous arch that is being considered.
· should permit immediate differentiation between the tooth-
supported and the tooth- and tissue-supported removable
partial denture.
· should be universally acceptable.
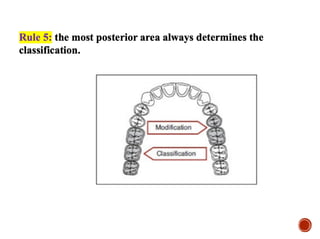
10.
· To assistour management of partially edentulous patients
· Many classifications have been proposed but Kennedy
classification is the most widely accepted
11.
Loading…
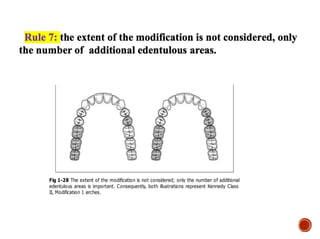
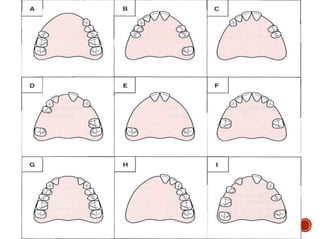
· Was proposedby Dr. Edward Kennedy in 1925
· Like Bailyn & Skinner classification, it classifies the partial
edentulous arches in a manner that suggests principles of design
for a given situation
· Kennedy classified the partial edentulous arches into four basic
classes
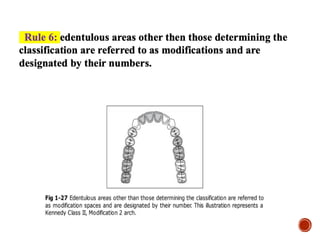
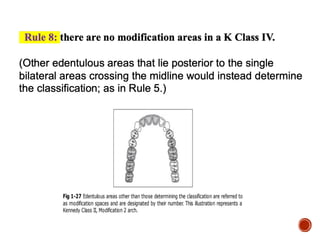
· The other edentulous areas that donot determine the class are
considered as modification spaces
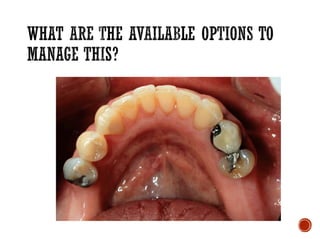
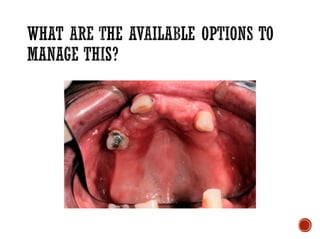
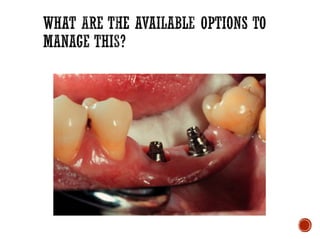
27.
1. An implant-supportedfixed partial denture
2. A tooth-supported fixed partial denture (FPD)
3. A removable partial denture (RPD)
4. No replacement
29.
Loading…
· If apatient presents with a long-standing edentulous space
into which there has been little or no drifting or elongation of
the adjacent or opposing teeth, the question of replacement
should be left to the patient's wishes.
· If the patient perceives no functional, occlusal, or esthetic
impairment, it would be a dubious service to place a
prosthesis.*
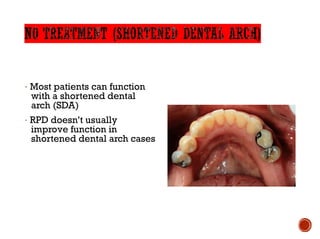
30.
· Most patientscan function
with a shortened dental
arch (SDA)
· RPD doesn’t usually
improve function in
shortened dental arch cases
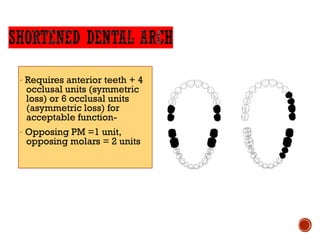
31.
· Requires anteriorteeth + 4
occlusal units (symmetric
loss) or 6 occlusal units
(asymmetric loss) for
acceptable function-
· Opposing PM =1 unit,
opposing molars = 2 units
32.
A removable partialdenture should be
considered only when a fixed restoration (either
tooth-supported or implant-supported) is
contraindicated
33.
·
·Edentulous spaces greaterthan two posterior teeth,
anterior spaces greater than four incisors, or spaces that
include a canine and two other contiguous teeth; i.e,
central incisor, lateral incisor, and canine; lateral incisor,
canine, and first premolar; or the canine and both
premolars.
34.
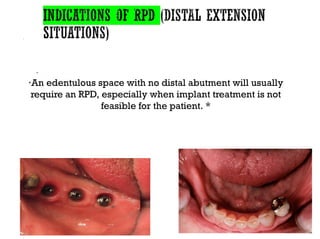
·
·An edentulous spacewith no distal abutment will usually
require an RPD, especially when implant treatment is not
feasible for the patient. *
35.
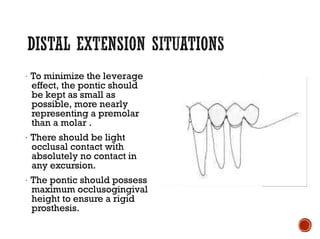
· To minimizethe leverage
effect, the pontic should
be kept as small as
possible, more nearly
representing a premolar
than a molar .
· There should be light
occlusal contact with
absolutely no contact in
any excursion.
· The pontic should possess
maximum occlusogingival
height to ensure a rigid
prosthesis.
36.
·Replacement of teethafter recent extractions often
cannot be accomplished satisfactorily with a fixed
restoration. When relining will be required later or when
a fixed restoration using natural teeth or implants will be
constructed later, a temporary RPD can be used.
37.
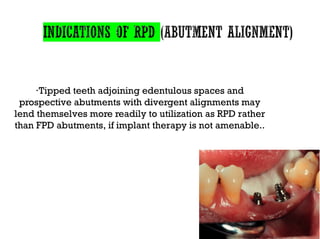
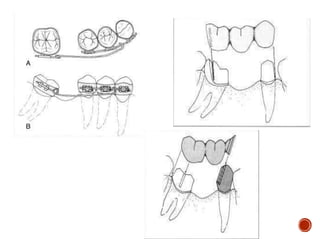
·Tipped teeth adjoiningedentulous spaces and
prospective abutments with divergent alignments may
lend themselves more readily to utilization as RPD rather
than FPD abutments, if implant therapy is not amenable..
39.
·
·Periodontally weakened primaryabutments may serve
better in retaining a well designed removable partial
denture than in bearing the load of a fixed partial denture.
*
41.
·
·Teeth with shortclinical crowns or teeth that are just
generally short usually will not be good FPD abutments.
·Unusually sound abutment teeth
42.
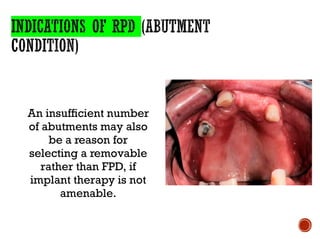
An insufficient number
ofabutments may also
be a reason for
selecting a removable
rather than FPD, if
implant therapy is not
amenable.
43.
·
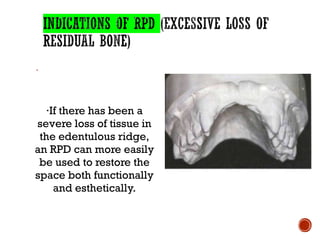
·If there hasbeen a
severe loss of tissue in
the edentulous ridge,
an RPD can more easily
be used to restore the
space both functionally
and esthetically.
45.
·
·Economics should notbe the sole criterion in arriving at a
method of treatment.
·When for economic reasons, complete treatment is out of
the question and yet replacement of missing teeth is
indicated, the restorative procedures dictated by these
considerations must be described clearly to the patient as a
compromise and not representative of the best that modern
dentistry has to offer. *
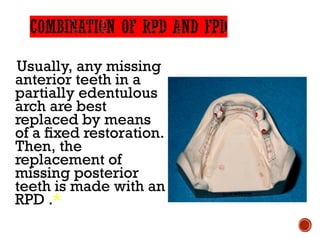
46.
Usually, any missing
anteriorteeth in a
partially edentulous
arch are best
replaced by means
of a fixed restoration.
Then, the
replacement of
missing posterior
teeth is made with an
RPD .*
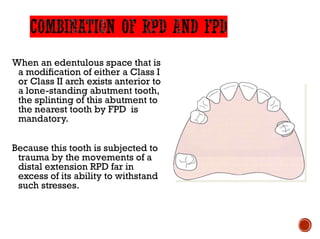
47.
When an edentulousspace that is
a modification of either a Class I
or Class II arch exists anterior to
a lone-standing abutment tooth,
the splinting of this abutment to
the nearest tooth by FPD is
mandatory.
Because this tooth is subjected to
trauma by the movements of a
distal extension RPD far in
excess of its ability to withstand
such stresses.
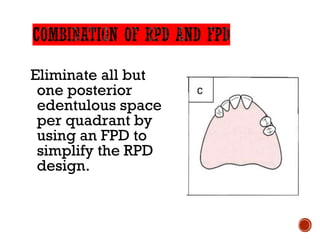
48.
Eliminate all but
oneposterior
edentulous space
per quadrant by
using an FPD to
simplify the RPD
design.
49.
· Dry mouthpoor RPD risk
· Limited patient finances
· Acceptable oral hygiene
· Reliable recall candidate
· Treatment simplification
· Advanced age
· Systemic health problems
· More adaptable to
dentition in transition to
edentulous state
50.
· Dry mouthhigh caries risk
· Muscular discoordination
· Mandibular tori
· Palatal soft tissue lesions
· Large tongue
· Exaggerated gag reflex
· Unfavorable attitude
toward RPD
· Patient can't cope with
aging, tooth loss
· Favorable opposing
occlusion
· Periodontally weakened
natural dentition may
permit FPD in less than
optimal situations
51.
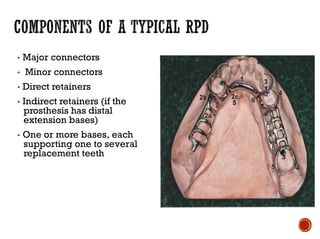
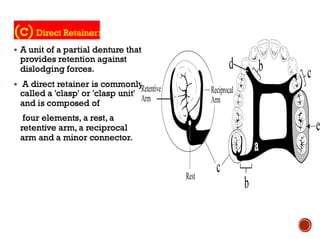
▪ Major connectors
▪Minor connectors
▪ Direct retainers
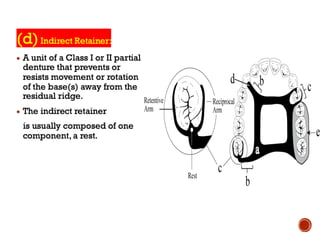
▪ Indirect retainers (if the
prosthesis has distal
extension bases)
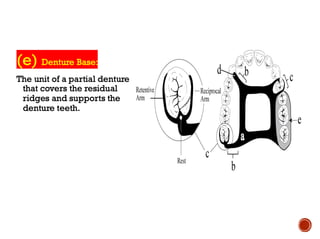
▪ One or more bases, each
supporting one to several
replacement teeth
57.
· McCracken’s RemovableProsthodontics,
13th Edition 2005 by McGivney GP, Carr
AB. Chapter 2 and 3
· McCracken’s Removable Prosthodontics,
13th Edition 2005 by McGivney GP, Carr
AB. Chapter 12 Diagnosis and Treatment
Planning P 178-183









































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


