P. Clinical toxicology
syllabus
1.General Principles of Toxicology
2. Drug toxicity
a. Acetaminophen poisoning.
b. Opiate poisoning.
c. Aspirin Poisoning.
d. Theophylline Poisoning.
3. Digoxin Toxicity
4. Determination of LD50
5. Guidelines for Seminar
Presentations:
a. CCl4
b. Ethanol and methanol
c. Cyanide and carbon monoxide
d. Organophosphorus and Organochlorine
3.
• clinical toxicology:Area of professional of medical
science (clinic) concerned with disease or poisoning by
toxic substance and its treatment.
• Poisons: Are chemicals or chemical products that are
distinctly harmful to humans.
• Toxin: It originally referred to a poison of animal or
plant origin.
• Toxidrome: A group of signs and symptoms and/or
characteristic effects associated with exposure to a
particular substance.
4.
How does thepoisoned patient die?
1. Depress the central nervous system (CNS).
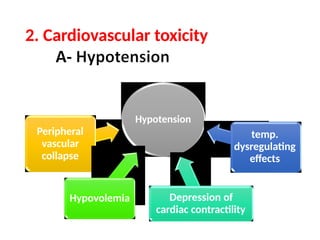
2. Cardiovascular toxicity.
3. Cellular hypoxia.
4. Seizures, muscular hyperactivity
5. Other organ system damage.
6. Traumatic injury.
5.
1. Depression of(CNS)
Overdoses
• barbiturates
and
alcohol
airway
obstruction
• by the flaccid
tongue
die
e.g. Narcotics and sedative-hypnotic drugs
• Occur inspite of adequate ventilation and oxygen
administration in case of poisons that interfere
with transport or utilization of oxygen e.g.
1. Cyanide.
2. Carbon monoxide.
9.
• Seizures maycause:
1. Pulmonary aspiration.
2. hypoxia.
3.Brain damage.
• Sustained muscular hyperactivity can lead to:
4. Hyperthermia
5. Muscle breakdown.
6. Myoglobinuria.
7. Lactic acidosis.
10.
• Behavioral effectsof ingested drug may result
in traumatic injury.
• e.g intoxication with alcohol and other
sedative-hypnotic drugs is a common
contributing factor to motor vehicle accidents.
11.
1. pulmonary fibrosis:
•Paraquat attacks lung tissue beginning
after several days of ingestion.
2. hepatic necrosis:
poisoning by acetaminophen or certain
mushrooms results in hepatic
encephalopathy and death 48-72 h.
12.
• Initial managementof the
poisoned patient
• Patient with coma, seizures, or otherwise
altered mental status should follow the
same approach regardless of the poison
involved.
13.
• Attempting tomake a specific
toxicological
diagnosis
supportive
delays
measures
the application
of that
form the basis
("ABCDs") of poisoning treatment.
14.
• A= airway:should be cleared of vomitus or any
other obstruction& oral airway or
endotracheal tube inserted if needed.
• B= Breathing: assessed by observation by oximetry,
measuring arterial blood gases.
15.
• C= circulation:monitoring of pulse rate, BP, urinary
output, evaluation of peripheral perfusion.
• Ds = Dextrose: Alcoholic or malnourished patients
should also receive 100 mg of thiamine I.M or in
I.V infusion solution at this time to prevent
Wernicke's syndrome.
16.
Assessment &management:
1. Clinicalassessment: all what mention previous.
2. Laboratory assessment
A-Liver function tests: Acetaminophen.
B- Renal function tests: NSAIDs.
C- ECG: Digoxin toxicity.
17.
D-Imaging findings
• Aplainfilm of abdomen useful in tablets,
e.g. iron and potassium, may be radiopaque.
• Chest radiographs reveal aspiration pneumonia,
hydrocarbon pneumonia, pulmonary edema.
• (CT) is recommended when head trauma
is suspected,
18.
E. Toxicology ScreeningTests:
Benefit:
Help in confirming a suspected intoxication or for
ruling out intoxication as a cause of apparent brain
death.
But: It is time consuming, expensive, and often
unreliable.
Note: They should not delay needed
treatment.
19.
Goals of treatment:
1.Reduce absorption of the toxin.
2. Enhance elimination.
3. Neutralize toxin.
20.
1. Reduce absorptionof the
toxin
Removal from surface skin and eye (wash
with soap and water).
Emesis induction
Gastric lavage
Activated charcoal administration.
Dilution - milk/other drinks for corrosives
Endoscopic or surgical removal of
ingested chemical
21.
2. Enhance
elimination
Keep agood urine output 150-200 ml/hr
Alkalinization of urine for salicylate and
phenobarbital poisoning, achieved by IV dose of
bicarb.
Hemodialysis.
22.
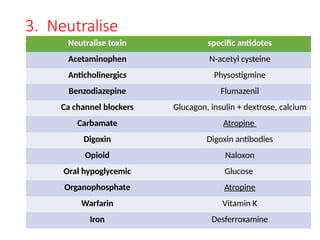
3. Neutralise
toxin Neutralisetoxin specific antidotes
Acetaminophen N-acetyl cysteine
Anticholinergics Physostigmine
Benzodiazepine Flumazenil
Ca channel blockers Glucagon, insulin + dextrose, calcium
Carbamate Atropine
Digoxin Digoxin antibodies
Opioid Naloxon
Oral hypoglycemic Glucose
Organophosphate Atropine
Warfarin Vitamin K
Iron Desferroxamine
























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










