Approach to SnakeBite
Presented by:
Dr Mohit Goyal
Moderator:
Dr Sanjeev Sharma
2.
Epidemiology
• Worldwide (approx.)
•50 lakh snake bites per year
• 1 lakh deaths per year
• India (approx.)
• 28 lakh snake bites per year
• 50 thousand deaths per year (0.5% of all deaths)
• 97% deaths in rural area and only 3% in hospital (2005 data)
https://www.who.int/snakebites/epidemiology/en/
3.
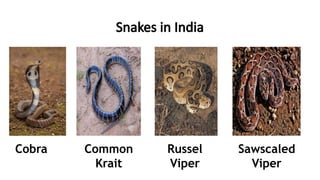
Venomous snakes inIndia
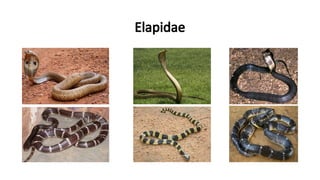
• Elapidae
• Common spectacled cobra, north Indian cobra, King cobra
• Common krait, banded krait, Sind krait
• Viperidae
• Typical vipers: Russell’s viper, saw-scaled viper, blunt nosed viper
• Pit vipers: Hump nosed pit viper, Indian bamboo viper
• Hydrophiidae: sea snakes
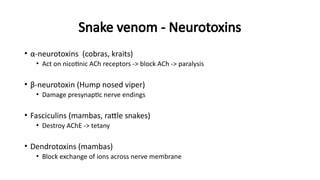
Signs & Symptoms
•Examine the bite site and look for fang marks, or any signs of local
envenomation.
• Fang mark or their patterns have no role to determine whether the
biting species was venomous or non venomous or amount of venom
injected, severity of systemic poisoning and nature of poisoning.
• Some species like Krait may leave no bite marks.
16.
• Asymptomatic (i.enon Venom related symptoms)
• Patients many a times present with nonspecific symptoms related to
anxiety.
• Dry Bite :
• Bites by nonvenomous snakes are common and bites by venomous
species are not always accompanied by the injection of venom.
• The percentage of dry bites ranges from 10–80% for various
poisonous snakes.
17.
• Neuroparalytic (Progressiveweakness; Elapid envenomation):
• These symptoms can be remembered as 5Ds and 2Ps :
• 5 Ds – Dyspnea, Dysphonia, Dysarthria, Diplopia, Dysphagia
• 2 Ps – Ptosis, Paralysis
• In chronological order of appearance of symptoms are:
• furrowing of forehead, Ptosis (drooping of eyelids) occurs first.
• followed by Diplopia (double vision),
• then Dysarthria (speech difficulty),
• then Dysphonia (pitch of voice becomes less)
• followed by Dyspnoea (breathlessness) and
• Dysphagia (Inability to swallow) occurs.
18.
• All thesesymptoms are related to 3rd, 4th, 6th and lower cranial nerve
paralysis.
• Finally, paralysis of intercostal and skeletal muscles occurs in
descending manner.
• To identify impending respiratory failure bedside lung function test:
• Single breath count –>30 is normal
• Breath holding time – normal > 45 sec
• Cry in a child whether loud or husky can help in identifying
impending respiratory failure.
19.
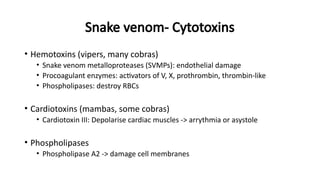
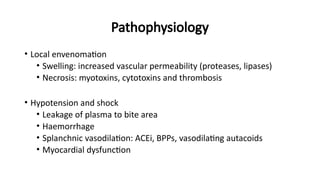
• Vasculotoxic:
• Dueto Viper species.
• Local manifestations –
• Russel’s viper > Saw scaled viper > Pit viper bite.
• Local swelling, bleeding, blistering, and necrosis.
• May progress to compartment syndrome.
• Systemic manifestations :
• Visible systemic bleeding from the action of haemorrhagins,
• Bleeding from pre-existing conditions e.g. haemorrhoids,
• Lateralizing neurological symptoms such as asymmetrical pupils may
be indicative of intra-cranial bleeding.
21.
• Myotoxic:
• Thispresentation is common in Sea snakebite.
• Patient presents with:
• Muscle aches, muscle swelling, involuntary contractions of muscles.
• Passage of dark brown urine.
• Cardiac arrhythmias due to hyperkalaemia, acute kidney injury due
to myoglobinuria, and subtle neuroparalytic signs.
22.
• Occult snakebite:
•Krait bite victims often present in the early morning with paralysis
with no local signs.
• Krait has nocturnal habitat and has fine slender teeth. Hence bite
marks usually cannot be identified even on close examination.
• Typical presenting history is that the patient was healthy at night, in
the morning gets up with severe epigastric/umbilical pain , followed
by typical neuroparalytic symptoms within next 4- 6 hours. There is
no history of snakebite.
23.
• Early morningsymptoms of acute pain abdomen with or without
neuroparalysis can be mistaken for a acute appendicitis, acute
abdomen, stroke, GB syndrome, myasthenia gravis and hysteria.
• Krait bite envenoming is diagnosed by developing descending
neuroparalysis while GB syndrome is by ascending paralysis.
• Strong clinical suspicion and careful examination can avoid not only
costly and unnecessary investigations ,but also help in avoiding undue
delay in initiation of a specific treatment with ASV.
24.
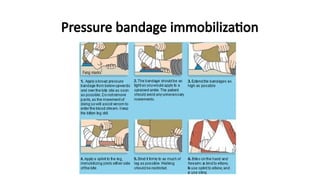
First aid andtransport
• Immobilization of patient and bitten limb
• No incisions, rubbing, vigorous cleaning, massage, herbal compounds
• Strict NO to tight tourniquets*
• DO NOT attempt to kill the snake
• Transport quickly, safely and comfortably
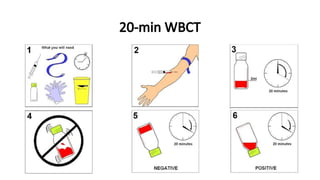
20-min WBCT
• Falsepositive results
• Syringes, plastic or polystyrene or polypropylene vessels
• Glass bottle cleaned with soap, detergent or is wet
• Antibiotic bottles cleaned with normal saline and hot air dried
• False negative results
• Early stages
• Plasma fibrinogen >0.5g/L
30.
Anti-snake venom
• Equineor sheep immunised by snake venom
• Monovalent or polyvalent
• Para-specific activity
• In India
• Polyvalent
• Equine
• Pepsin refined F(ab’)2 fragment of IgG
• Indian cobra, common krait, Russell’s viper, saw-scaled viper
31.
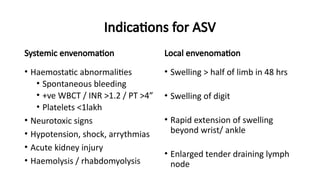
Indications for ASV
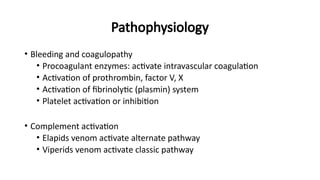
Systemicenvenomation
• Haemostatic abnormalities
• Spontaneous bleeding
• +ve WBCT / INR >1.2 / PT >4”
• Platelets <1lakh
• Neurotoxic signs
• Hypotension, shock, arrythmias
• Acute kidney injury
• Haemolysis / rhabdomyolysis
Local envenomation
• Swelling > half of limb in 48 hrs
• Swelling of digit
• Rapid extension of swelling
beyond wrist/ ankle
• Enlarged tender draining lymph
node
32.
Timing of ASV
•As early as possible
• Can reverse systemic envenomation up to 2 or more weeks
• As long as coagulopathy persists
• Inappropriate use of ASV STRONGLY DISCOURAGED
• NO ABSOLUTE contraindications
33.
Route of administration
•Intravenous route
• ASV supplied in dry powder form has to be
reconstituted by diluting in 10 ml of distilled
water/normal saline
• Mixing is done by swirling and not by vigorous
shaking.
• Slow IV push: maximum 2ml/minute
• Local administration of ASV NOT RECOMMENDED
34.
Dose of ASV
•Dose of ASV for neuroparalytic snakebite:
• ASV 10 vials stat as infusion over 30 minutes followed by 2nd dose of
10 vials after 1 hour if no improvement within 1st hour.
• Dose of ASV for vasculotoxic snakebite :
• Two regimens low dose infusion therapy and high dose intermittent
bolus therapy can be used.
• Low dose infusion therapy is as effective as high dose intermittent
bolus therapy .
35.
• Low Doseinfusion therapy:
• 10 vials for Russel’s viper or 5 vials for Saw scaled viper as stat as
infusion over 30 minutes
• followed by 2 vials every 6 hours as infusion in 100 ml of normal
saline till clotting time normalizes or for 3 days whichever is earlier.
• High dose intermittent bolus therapy:
• 10 vials of polyvalent ASV stat over 30 minutes as infusion, followed
by 6 vials 6 hourly as bolus therapy till clotting time normalizes
and/or local swelling subsides.
• No ASV for Sea snakebite or pit viper bite as available ASV does not
contain antibodies against them.
36.
Max Dose ofASV
• The range of venom injected is 5 mg-147 mg. The total required dose
range between 10 and 30 vials as each vial neutralizes 6 mg of
Russell’s Viper venom. Depending on the patient condition, additional
vials can be considered.
• Ptosis in Common Krait bite is due to presynaptic blockage, further
ASV and Neostigmine dose beyond 3 doses cannot reverse it, since
regeneration is a natural process and may take 4-5 days.
• Both ASV and Neostigmine injection should be stopped when the
initial syndrome of pharyngeal muscle palsy is over.
37.
Special Population
• ASVdose in pregnancy:
• Pregnant women are treated in exactly the same way as other
victims. The same dosage of ASV is given. Refer the victim to a
gynecologist for assessment of any impact on the foetus.
• ASV dose in children:
• Children also are given exactly the same dose of ASV as adults as
snakes inject the same amount of venom into children and adult.
• However, reduce amount of fluid in running bottle to 200 ml to
avoid fluid over load.
38.
Special Population
• Victimswho arrive late:
• Sometimes victims arrive late after the bite, often after several days,
usually with acute kidney injury.
• Determine current venom activity such as bleeding in case of viperine
envenomation.
• Perform 20WBCT and determine if any coagulopathy is present then
administer ASV.
• If no coagulopathy is evident, treat kidney injury, if any.
39.
Indications for repeatASV
• Persistence or recurrence of bleeding after 1-2 hours
• Blood incoagulability after 6 hours
• Deteriorating neurological signs after 1 hour
• Worsening cardiovascular signs after 1 hour
• Dose of repeat ASV
• Neurological signs: up to 20 vials
• Coagulopathy: usually 30 vials
40.
• Administer followingin addition:
• Oxygen
• Assisted ventilation : usually short since neuroparalysis reverses
quickly with prompt administration of ASV.
• Administer ‘Atropine Neostigmine (AN)’ schedule
MANAGEMENT NEUROTOXIC
(NEUROPARALYTIC) ENVENOMATION
41.
Atropine neostigmine (AN)dosage schedule
1. Atropine 0.6 mg followed by Neostigmine 1.5mg to be given IV stat
2. Repeat dose of neostigmine 0.5 mg with atropine every 30 minutes for 5
doses.
3. Thereafter to be given as tapering dose at 1 hour, 2 hour, 6 hours and 12
hour.
• Majority of patients improve within first 5 doses.
• Positive response to “AN” trial is measured as 50% or more recovery of
the ptosis in one hour.
42.
• Stop Atropineneostigmine (AN) dosage schedule if:
• Patient has complete recovery from neuroparalysis.
• Patient shows side effects in the form of fasciculations or bradycardia.
• If there is no improvement after 3 doses.
• Improvement indicates Cobra bite.
• No improvement - probable Krait bite.
• Krait affects pre-synaptic fibres where calcium ion acts as neurotransmitter
• Give Inj. Calcium gluconate 10ml IV slowly over 5-10 min every 6 hourly and
continue till neuroparalysis recovers which may last for 5-7 days.
43.
• Strict bedrest to avoid even minor trauma.
• Screen for hematuria, hemoglobinuria, myoglobinuria by Dipstick
method.
• Centrifuged urine showing pink color indicates hemoglobinuria, clear
supernatant (RBCs settle down as deposit) indicates myoglobinuria.
• Closely monitor urine output and maintain 1 ml/kg/h urine output.
MANAGEMENT OF VASCULOTOXIC SNAKEBITE:
44.
SUPPORTIVE TREATMENT
• Forcoagulopathy:
• If not reversing after 2-3 doses of ASV administration ,then
clotting factors should be replaced using – Fresh Frozen Plasma
and a PCV fall of<30% necessitates blood transfusion .
• Avoid I.M. injections.
• Early FFP administration (< 6-8hours) post-bite is less effective.
• FFP @ 10-15 ml/kg B.W over 30-60min within 4 hours of
administration of ASV is proven effective with an aim to restore
coagulation function (INR <2.0) , at 6hour post ASV administration.
45.
• For hypotensionand shock:
• Give fluid challenge: An adult patient can be given two litres of
isotonic saline over one hour or until the jugular venous
pressure/central venous pressure has risen to 8-10 cm above the
sternal angle (with the patient propped up at 45degree).
• Stop immediately if pulmonary odema develops.
• In sepsis, noradrenaline is the inotropic agent of choice.
46.
• For AKI:
•Forced Alkaline Diuresis
• If the patient has oliguria or dipstick positive for blood give a trial of
forced alkaline diuresis (FAD) within first 24 hours of the bite to
avoid pigment nephropathy leading to acute tubular necrosis (ATN).
• Delayed FAD has no role.
47.
• Sequence ofFAD in adults is as follows:
1. Inj. Frusemide 40 mg IV stat
2. Inj. Normal saline 500 ml + 20 ml of NaHCO3 over 20 minutes
3. Inj. Ringer’s lactate 500 ml + 20 ml of NaHCO3 over 20 minutes
4. Inj. 5% dextrose 500 ml + 10 ml of Potassium Chloride over 90
minutes
5. Inj. Mannitol 150 ml over 20 min – Whole cycle completes in 2 h
30 min and urine output of 3 ml/min is expected.
48.
• If patientresponds to first cycle continue for 3 cycles.
• FAD converts oliguria into polyuria and avoid ATN and acute kidney
injury needing dialysis in more than 75% patients.
• If there is no response to furosemide discontinue FAD and refer
patient immediately for dialysis.
49.
ASV reactions
• Earlyanaphylactic reactions (minutes to 3 hours)
• Urticaria, dry cough, fever, vomiting, diarrhoea, pain abdomen,
tachycardia, hypotension, bronchospasm, angio-edema
• Mechanisms:
• Complement activation by IgG aggregates or Fc fragments
• Mast cell or basophil activation by antivenom proteins
• Skin and conjunctival hypersensitivity tests not recommended
50.
ASV reactions
• Treatment
•Stop ASV infusion
• Adrenaline: 0.5ml (1 in 1000) IM, q 5-10 min
• IV adrenaline: 1mg (1 in 1000) in 250ml D5% or NS (1-4ug/min)
• Anti-histamine (H1) / Inhaled SABA
• Leg elevation / Intravenous fluids
• Prophylaxis
• 0.25 ml (1in 1000) adrenaline IM before ASV
• Anti-histamine, GCs and rate of infusion do not effect reactions
51.
ASV reactions
• Pyrogenic(endotoxin) reactions (1-2 hours)
• Chills / rigors, fever, vasodilation, hypotension, febrile seizures
• Pyrogen contamination during manufacture
• Rx: Paracetamol
• Late (serum sickness like) reactions (1-12 days)
• Fever, nausea, vomiting, diarrhoea, itching, urticaria, arthralgia,
myalgia, lymphadenopathy, periarticular swelling, mononeuritis,
proteinuria, IC nephritis, encephalopathy
• Rx: 5 day course of anti-histamine or prednisolone
52.
Supportive treatment
• Mechanicalventilation
• FFP and clotting factor transfusion
• Anticholinesterase drugs useful in cobra bites
• Crystalloids infusion
• Vasopressors infusion
• Renal replacement therapy
• Target urine output 200-300 ml/hour in haemolysis / rhabdomyolysis
• ABG and heparin are contraindicated in coagulopathy
53.
Local wound management
•Antibiotics
• Amoxycillin + clavulanic acid
• Pipercillin + tazobactum
• Ciprofloxacin
• 3rd
gen. cephalosporins
• TETANUS TOXOID IS MUST
• Debridement of necrotic tissue
• Fasciotomy for compartmental syndromes
54.
Compartment syndrome
• Itis rare and difficult to diagnose clinically because several
features of local Envenoming overlaps.
• Compartment syndrome is diagnosed with 5 ‘P’ –
1. Pain (severe)
2. Pallor
3. Paraesthesia
4. Pulselessness
5. Paralysis or weakness of compartment muscle.
55.
Criteria for fasciotomyin snakebite limb:
• Haemostatic abnormalities have been corrected.
• Clinical evidence of an intracompartmental syndrome .
• Intra-compartmental pressure >40 mmHg of normal saline (in
adults).
• This can be confirmed by vascular Doppler and rising CPK in
thousands.
• Timely fasciotomy decreases the need for repeated dialysis.
56.
When to discharge?
•If no symptoms and signs develop after 24 hours the patient can be
discharged.
• Keep the patient under observation for 48 hours if ASV was infused.
57.
Follow up
• Warningsigns explained
• Return to the emergency if:
• evidence of bleeding.
• worsening of pain and swelling at the site of bite.
• difficulty in breathing, altered sensorium,
• reduced or increased urine output etc.
• Explain about the signs and symptoms of serum sickness (fever, joint
pain, joint swelling) which may manifest after 5-10 days.
References
• Guidelines forthe management of snake bites – 2nd
edition, 2016;
WHO regional office for south-east Asia
• Standard treatment guidelines- snakebite, 2016; DGHS, MoHFW, GOI
• Surjit Singh and Gagandeep Singh. Snake bite: Indian guidelines and
protocol. Medicine Update, 2013