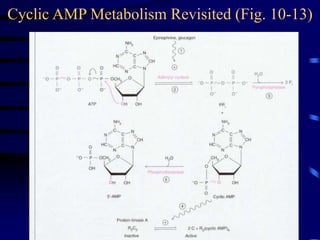
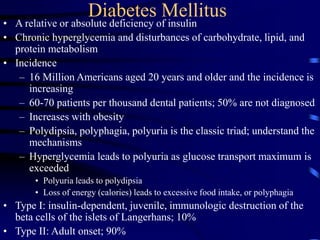
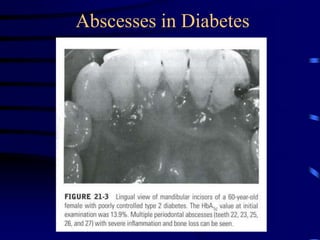
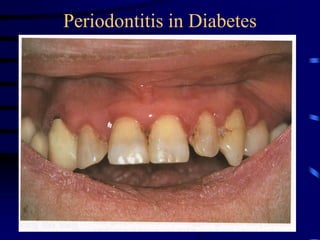
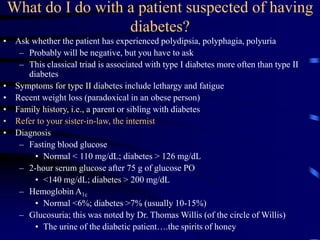
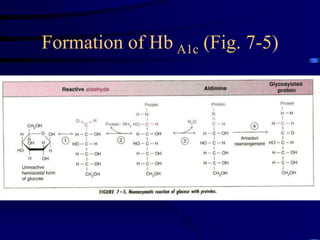
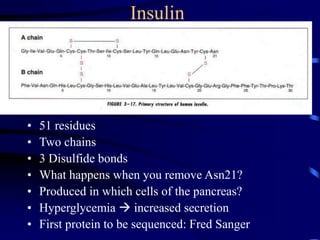
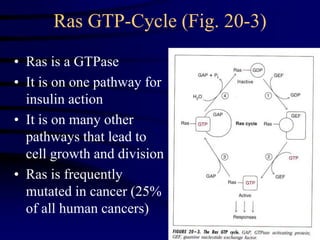
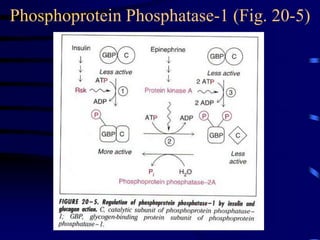
The document provides an overview of hormones' roles in regulating adenylyl cyclase activity, insulin action, and diabetes mellitus, including the mechanisms of hyperglycemia and the differences between type I and type II diabetes. It discusses the physiological mechanisms linking glucagon and insulin signaling pathways, their effects on glycogen metabolism, and the consequences of diabetes on health. Additionally, the document covers treatment approaches for diabetic hypoglycemia and the impact of insulin on glucose uptake and metabolism.

![Diabetes: the Glucagon/Insulin Ratio
• Glucagon
– Produced by the alpha cells of the islets of Langerhans
– Early preparations of “insulin” produced hyperglycemia followed by
hypoglycemia
• The hyperglycemic factor represented contamination
• This factor was purified, characterized, and re-named glucagon
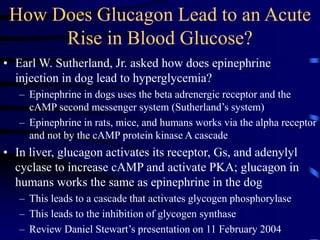
– It produces hyperglycemia by at least three mechanisms
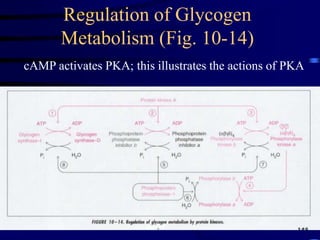
• It promotes glycogen breakdown as noted above
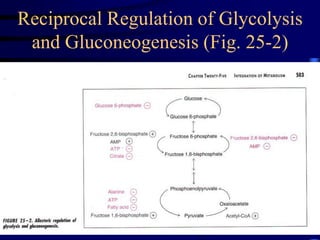
• It inhibits glycolysis and increases gluconeogenesis
– cAMP activates PKA, which phosphorylates fructose-6-phosphate-2-
kinase/fructose-2,6-bisphosphatase
– This decreases [fructose-2,6-bisphosphate]
» This removes a stimulant of glycolysis at the PFK step
» This removes an inhibitor of gluconeogenesis at the fructose-1,6-
bisphosphatase step
• PKA promotes transcription of PEP carboxykinase, an important enzyme
in gluconeogenesis
– The high ratio of glucagon/insulin action promotes
hyperglycemia](https://image.slidesharecdn.com/dentalhormones04-240605064348-9a37e6c9/85/insulin-hormone-synthesis-moa-uses-adverse-effects-34-320.jpg)
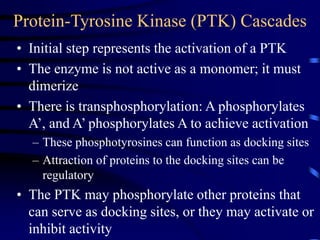
![Regulation
of [Fructose
2,6-BP]
• Glucagon increases cAMP and PKA activity
• PKA increases Frc 2,6 BPase activity and decreases
[Frc 2,6 BP]
• Glycolysis decreased, gluconeogenesis increased
Fig 7-11](https://image.slidesharecdn.com/dentalhormones04-240605064348-9a37e6c9/85/insulin-hormone-synthesis-moa-uses-adverse-effects-35-320.jpg)

















![anti diabetics [Autosaved] final.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/antidiabeticsautosavedfinal-231210163451-81c335f7-thumbnail.jpg?width=640&height=640&fit=bounds)


























![REF arr [Autosaved]dddddddddddddddddddd.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/refarrautosaved-250205075410-bd14ca78-thumbnail.jpg?width=640&height=640&fit=bounds)






















