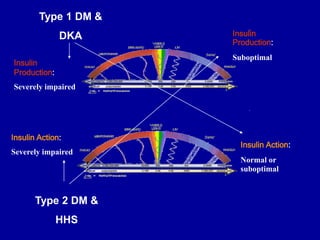
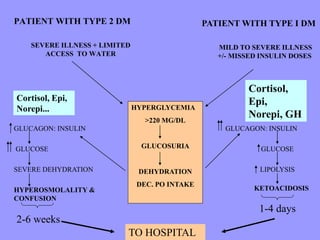
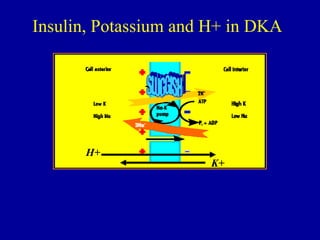
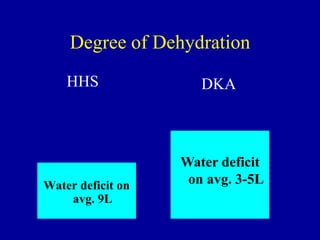
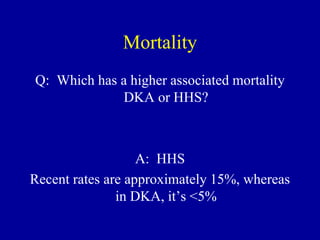
The document discusses hyperglycemic emergencies, specifically Diabetic Ketoacidosis (DKA) and Hyperglycemic Hyperosmolar State (HHS), including definitions, epidemiology, diagnoses, and management strategies. It emphasizes the rising prevalence of DKA and its implications for treatment, highlighting the need for aggressive fluid resuscitation and careful monitoring of potassium levels. The document also outlines the differing mortality rates associated with DKA and HHS, as well as the critical importance of identifying underlying illnesses in affected patients.


![How to measure metabolic acidosis?
• Blood pH: measures acidemia
• “Anion Gap”
– Normal extracellular anions =
• Measurable: Cl- and HCO3-
• Unmeasurable: proteins
– Normal measureable extracellular cation =
• Na++
– Electric “balance”
• Anions must =Cations
– Na++ - [Cl- + HCO3-] – (unmeasurable anions) = 0
The
normal
“Gap”](https://image.slidesharecdn.com/hypergcrisitnoonconference2013-240605050849-854ceeb1/85/Hyperglycemia-insulin-hyperglycemic-emergencies-26-320.jpg)














































![REF arr [Autosaved]dddddddddddddddddddd.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/refarrautosaved-250205075410-bd14ca78-thumbnail.jpg?width=640&height=640&fit=bounds)






















