

More Related Content
What's hot
What's hot (20)
Infeksionet odontogjene -Dr.Albin Maksuti
- 2. Përkufizimi : mes m.levator labi superior dhe m.levator anguli oris m.levator ang oris2Albin Maksuti
- 3. • Infeksion odontogjenë(kanini,paramolari) • Cistat e infektuara,Sinusitet,Furunculus 3Albin Maksuti
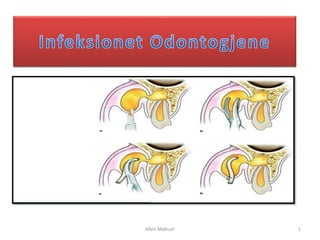
- 4. Manifestohet me edeme te shprehur ne regjion infraorbital, e cila shkelqen,e skuqur Prek kapakun e poshtem te syrit,anen mediale te hundes Ka humbje te sulkusit nasolabial Ne palpim: E ndjeshme ,fluktuon 4Albin Maksuti
- 5. • Kur infeksioni përparon në fazën kronike, mund të rezultojë me • Dhëmbi është i lëvizshëm dhe është i ndjeshem ne perkusion • Pasi eshte ne kend syrit rrezik per 5Albin Maksuti
- 6. Paralel me kreshten Alveolare Depertohet me Hemostat deri ne kontakte me kocken ,qe te zbrazet qelbi Vendoset Dreni qe perforcohet me suture Në drejtim te rrudhave natyrale ,rralle 6Albin Maksuti
- 7. Incizivi lateral, Kanini,PM, dhe me RR.P te M-1 7Albin Maksuti
- 8. Perkufizimi : • • Me pllaken kortikale te qiellzes se forte • • Me periostin dhe mukozen • Me kreshten alveolare te maksilles dhe dhembet 8Albin Maksuti
- 10. : 1) Osteomielitin 2) Cistat 3) Absceset 4) Tumoret 10Albin Maksuti
- 11. • Ne drejtim sagjital AP,duke shmang a.n.palatinus major • Mund te behet incizion sulkuror qe te shmang demtimet e tyre • Disa autore sugjeronje eksicizion te mukozes per drenazhe me te mire 11Albin Maksuti
- 12. Kufinjet: • M.ptergoid • Tuberi maksillar • Ramus Mandibule-m.temporal • Fosa pterygopalatina • Fossa infratemporale 3.Abscesi Retromaksillar 12Albin Maksuti
- 13. ETIOLOGJIA : Molaret • Infeksion ,Hematome Pasqyra Klinike: • Nuk ka shenja dukshme ekstraorale,pasi ne thellesi. • Manifestohet me dhembje te forta,Trizmus te forte,prani te skuqjes dhe edemes pas tuberit. • Nese edema mbi harkun zigomatik-dmth prekje hap.temporale,infratemporale Nese edema shtrihet kah kapaku syrit-dmth prekje e orbites(fossa pterygopalatina) 13Albin Maksuti
- 14. Prapa Crista Zygomatico Alveolare,ne nivel te M2-M3 Me Pean depertohet kah tuberi,dhe pas zbrazjes se qelbit vihet Dreni 14Albin Maksuti
- 15. m.buccinator,kend buzeve m.masster dhe pterigoid medialis m.zygomaticus major minor(procc.zygomatik) lekura,platizma(kufiri poshtem i Mandibules). m.buccinator 15Albin Maksuti
- 16. 16Albin Maksuti
- 17. ETIOLOGJIA: • Nese rrenjet e M poshtem gjenden mbi m.buccinator infeksioni ne vestibulum. • Nese RR e M poshtem gjenden nen infeksioni formohet ne hapesiren bukale. • Ne Maksille nese qelbi perforon kocken mbi ngjitjen e muskulit ,formohet abscesi ne hap.bukale. • Nese qelbi perforon kocken nen nivel ngjitjes se muskulit formohet abscesi submukozal. 17Albin Maksuti
- 18. Komunikimi me Hap.Fqinje • LARTE komunikon me: • POSHTE komunikon me: 18Albin Maksuti
- 19. PASQYRA KLINIKE Manifestohet me edeme e cila shtrihet nga kendi buzes deri ramus mandibule ,larte deri tek harku zigomatik poshte deri te baza mandibules Edema e dhembshme ne palpim,lekura e skuqur dhe shkelqen . Edema zgjerohet ne hap.submandibulare,submaseterike dhe temporale Trizmusi shfaqet veq kur te perhapet ne keto hapesira fqinje infeksioni Te pranishme edhe simp.pergjithshme sikurse temperature,zbehje ,ethe,leukocitoze dhe rritje e SE. 19Albin Maksuti
- 20. Dg Diferenciale : 20Albin Maksuti
- 21. MJEKIMI • Ne drejtim AP ne sulkusin bukal ,kujdes duc stenonit • Incizioni intra oral favorizohet shkak i estetikes,fluktuimit,dhe preventive ndaj lendimit te nervit • Ne tehun e poshtem te mandibules-paralel dhe poshte 2 cm. 21Albin Maksuti
- 22. ABSCESI SUBLINGUAL :Mukoza e dyshemese se gojes • : Mylohyoid muscle • Sip.Brendshme e Manbibules siper m.milohiod. :muskujte hyoglossus genioglossus and geniohyoid : Kocka Hyoide. 22Albin Maksuti
- 23. Gj.pshtymore sublinguale me kanalin e saj ekskretor a.n.lingualis n.sublingualis Parcialishte gj.submandibulare 23Albin Maksuti
- 24. Etiologjia : ( nga :I-K-PM dhe M-1 kur apekset i kane mbi ngjitjen e m.milohioid) infeksione kanal te gj.sublinguale,gure) si dhe nga sikurse submandibular,submental 24Albin Maksuti
- 25. • Manifestohet me shenjat e pergjithshme te infeksionit • Tipike Edema e kufizuar me dhembje ,ne presion e forte • Skuqje mukozes se dyshemese e cila eshte e ngritur mbi nivel tehut incizal • Gjuha e ngritur dhe anon kah ana e shendosh,larte dhe prapa,andaj ka levizshmeri te kufizuar te gjuhes,probleme ne te folur ,dhe disfagi • Kur nekroza prek m.milohiod infeksioni zgjerohet ne hap fqinje si submentale dhe submandibulare • Dg diferenciale me Cista dermoide/ epidermoide dhe Ranulen 25Albin Maksuti
- 26. • Paralel me dhembet,ne vendin me te shprehur te fluktuimit ne drejtim A-P ne sulcusin sublingual duke shmang duc.Warton dhe n.lingual,a.sublinguale. • Me rrallë: • Kur të dy hapësirat submentale dhe sublinguale përmbajnë qelb, ato mund të drenohen përmes incizionit në rajonin submental, duke depertue përmes muskulit mylohyoid. 26Albin Maksuti
- 27. : m.milohoid dhe m.hyoglossus Lekura,fascia qafes Venter anterior m. digastricus :Venter posterior m.digastricus,lig.stilohioid : Kufiri inferior corpus mandibula : m.venter ant m.digastricus 27Albin Maksuti
- 28. • Odontogjene (PM-M mandibular • Jo odontogjene(infeksionet purulente te gj.pshtymore) • HapesiratFqinje(sublingual,sub mental 28Albin Maksuti
- 29. • Tipike Edema e njeanshme ,ne regjion submandibular,e dhembshme ,lekura mbi edeme shkelqen. • E ndjeshme ne palpim • Trizmus i moderuar kur perfshin m.pterigoid medial • Dhembi shkaktare mund jete i ndjeshem ne palpim • Dg diferenciale me : • Linfadenitet ,semundjet e gj.pshtymore,limfomen Hodgkin,Tumoret Malinje etj 29Albin Maksuti
- 30. Mjekimi • Paralel me tehun e poshtem te mandibules 1cm ,kujdes a.n.v.facialis(incizioni prapa) • Depertohet me hemostat,vendoset dreni 3-6 dite. • Ordinohen antibiotike 30Albin Maksuti
- 31. Perkufizimi : • Sip mediale e Ramusit të mandibulës. m.pterygoid medial. Gjëndër parotide Rapha Pterygomandibular. Muskujt lateral pterygoid :mpterigoid medial • N.Lingualis, N.A V.alveolare inferior 31Albin Maksuti
- 32. Etiologjia 1. Odontogjene(Molaret,Pericor onitis 2. Jo-odontogjene(gjate anestezise bllok me gjilp.josterile) 3. Hematoma ,Lendimet 4. Cistat dhe Osteomielitis 5. Nga Hap.Fqinje(submandibular,inf ratemporal,laterale faringeale) 32Albin Maksuti
- 33. • Ekstraoral vrehet nje edeme e paket e ndjeshme tek angulusi • Intraoral –trizmus i forte,skuqja mukozes,edema,dislokim i uvules kah ana e shendoshe • Veshtiresi ne pertypje • Mund zgjerohet ne tehun e pasem te Ramus Mandibules-ne gj.parotide. • Mund pergjate m.temporal te perhapet ne hap.infratemporale dhe temporale • Mund zgjerohet ne hap.retromaxillare (tromboflebit) • Mund zgjerohet hap.submandibulare,faringeale 33Albin Maksuti
- 34. • INCIZION INTRAORAL • Ne anen e brendshme te Ramusit ,mbi trigonum Retromolare,depertohet me pean ne mes Ramusit dhe m.pterygoid medial. • Incizion i gjate 1.5 cm ,I thelle 4-5 cm • Tek Trizmuesi shprehur – incizion ekstraoral : 2 cm ne Bazen e Mandibules (nen angulus). • Antibiotik,lecka te ftohta. 34Albin Maksuti
- 35. 35Albin Maksuti
- 36. • muskulit mental siper dhe m.platizmes poshte I. Dhembet frontal(K) apex kur e kane nen m.mental-ashtu qe dhembi shkaktar eshte i ndjeshem II. Cistat e infektuara III. Traumat IV. Sialodenitis gj.submandibulare Ngjitjet e indeve te forta dhe perhapja radiale e indit lidhor e pengon perhapjen e inflamacionit 36Albin Maksuti
- 37. Ne drejtim te rrudhave ,ne vendin me te shprehur te fluktuimit,depertohet me pean ,vihet dreni Antibiotike Incizion INTRAORAL Behet nese absc.fluktuon intraoral ne vestibulum 37Albin Maksuti
- 38. Perkufizimi • Lozha submentale shtrihet mes m.milohioid dhe m.digastricus venter ant. • Perpara: Corpus Mandibula pjesa e brendshme • Pas:Kocka Hioide • Siper: m.milohioid • Poshte: platisma me Fascien • Lateral m.digastricus vent ant • Lozha tille permban : N.limfatike submentale Ind dhjamor ,lidhor gjendra etj. v.jugulare anterior 38Albin Maksuti
- 39. 1. Dh.frontal te poshtem 2. Traumat 3. Cistat e infektuara 4. Limfadenitis 5. Dhe ne menyre sekondare nga regj.submandibular dhe sublingual • Edeme e pakufizuar ne regj.submental –deri ne kocken hioide-andaj vrehet fenomeni mjekres se dyfishte • Edema e ndjeshme ne palpim dhe fluktuon • Lekura e skuqur • Dhembi shkaktar mund te jete I ndjeshem dhe i diskoloruar Cista Dermoide,Cista mediale Qafes ,Limfadenitet 39Albin Maksuti
- 40. • Preferohet terthorazi,ne drejtim sagjial shkak i estetikes,depertohet me pean –drenohet qelbi ,vihet dreni 3-5 dite jodoform gase • Ne drejtim horizontal paralel 40Albin Maksuti