What is Impulsivity?
•Rapid, unplanned reactions to stimuli before complete processing of information.
• Decreased sensitivity to negative consequences of behavior.
• Lack of regard for long-term consequences.
• Impulsivity often has an impact, not only on the impulsive individual, but also on
others.
[F. Gerard Moeller, Ernest S. Barratt,2001]
• Failure to inhibit behaviors motivated by reward.
[Grant et al.2006]
What is Compulsivity?
•Failure to suppress repetitive behaviors designed to relieve
tension or reduce a negative emotion state.
[Grant et al.2006]
• Desire to avoid harm.
[Fineberg et al., 2010]
7.
What is Spectrumdisorder?
“Not a unitary disorder but rather syndrome composed of subgroups”
• Includes a range of linked conditions
• The different elements of a spectrum either have a similar appearance or
are thought to be caused by the same underlying mechanism.
• Bipolar spectrum
• Schizophrenia spectrum
• Obsessive compulsive spectrum
8.
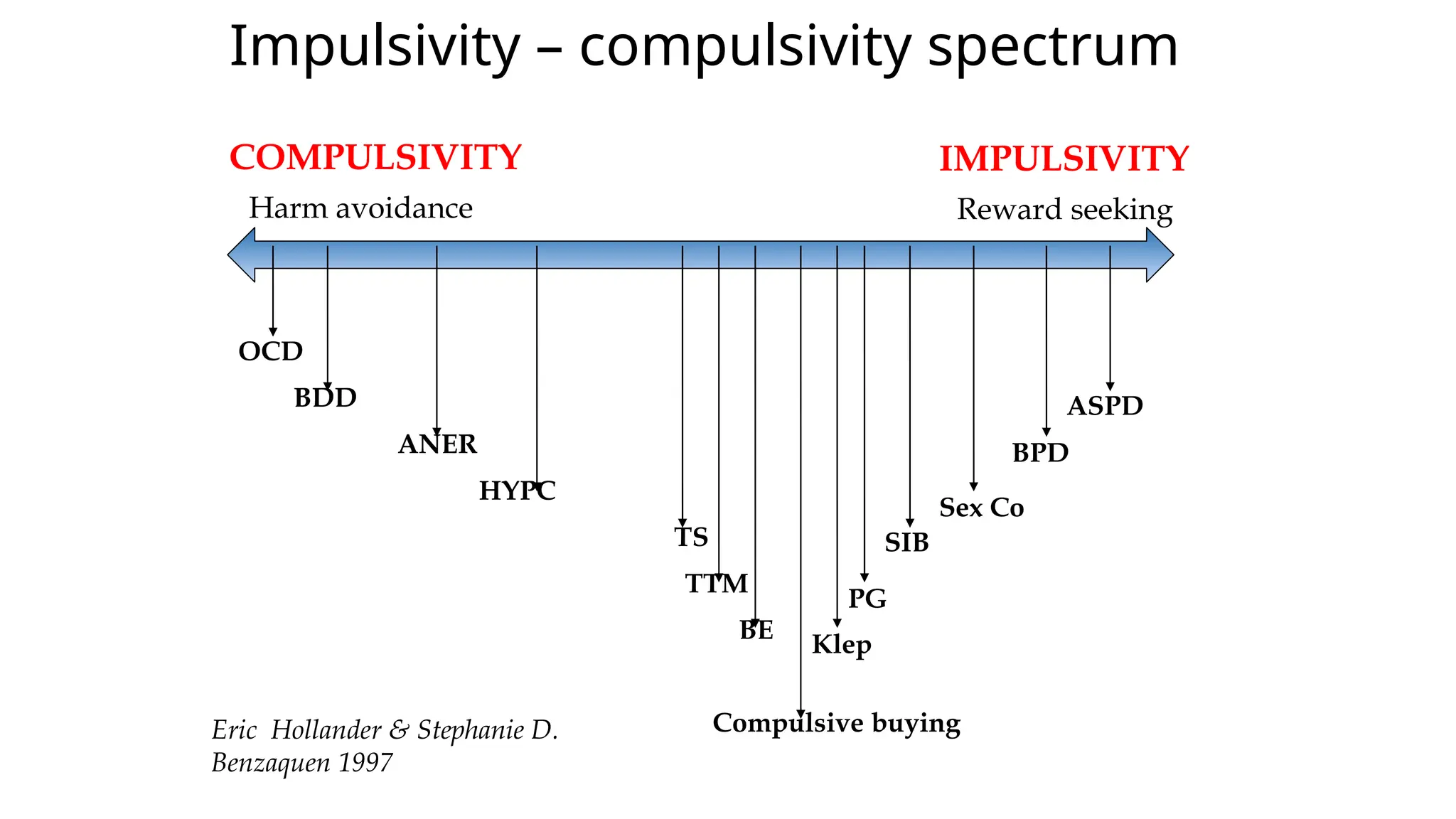
Impulsivity – compulsivityspectrum
IMPULSIVITY
Harm avoidance Reward seeking
COMPULSIVITY
OCD
BDD
ANER
HYPC
TS
TTM
BE
Compulsive buying
Klep
PG
SIB
Sex Co
BPD
ASPD
Eric Hollander & Stephanie D.
Benzaquen 1997
10.
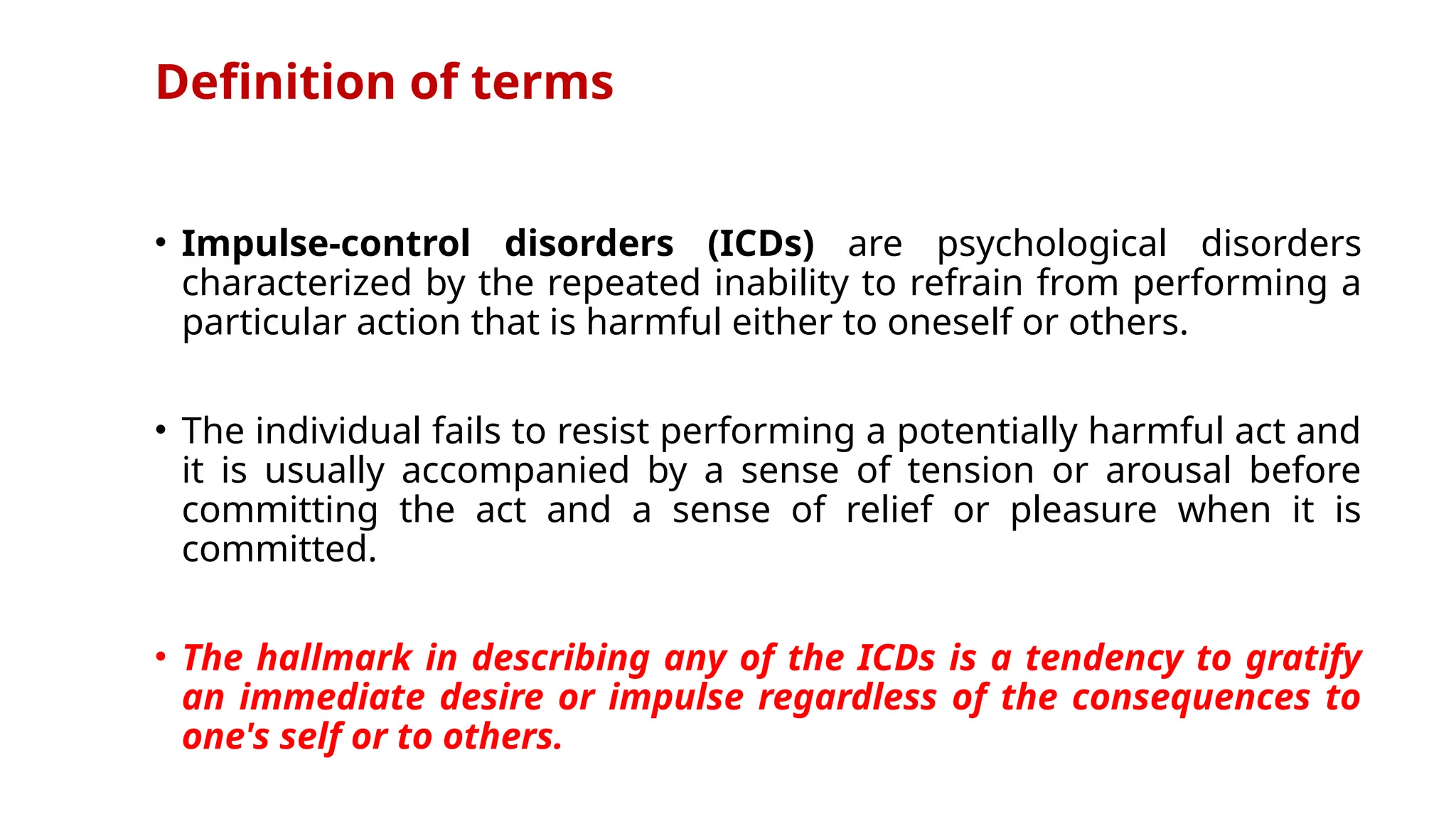
Definition of terms
•Impulse-control disorders (ICDs) are psychological disorders
characterized by the repeated inability to refrain from performing a
particular action that is harmful either to oneself or others.
• The individual fails to resist performing a potentially harmful act and
it is usually accompanied by a sense of tension or arousal before
committing the act and a sense of relief or pleasure when it is
committed.
• The hallmark in describing any of the ICDs is a tendency to gratify
an immediate desire or impulse regardless of the consequences to
one's self or to others.
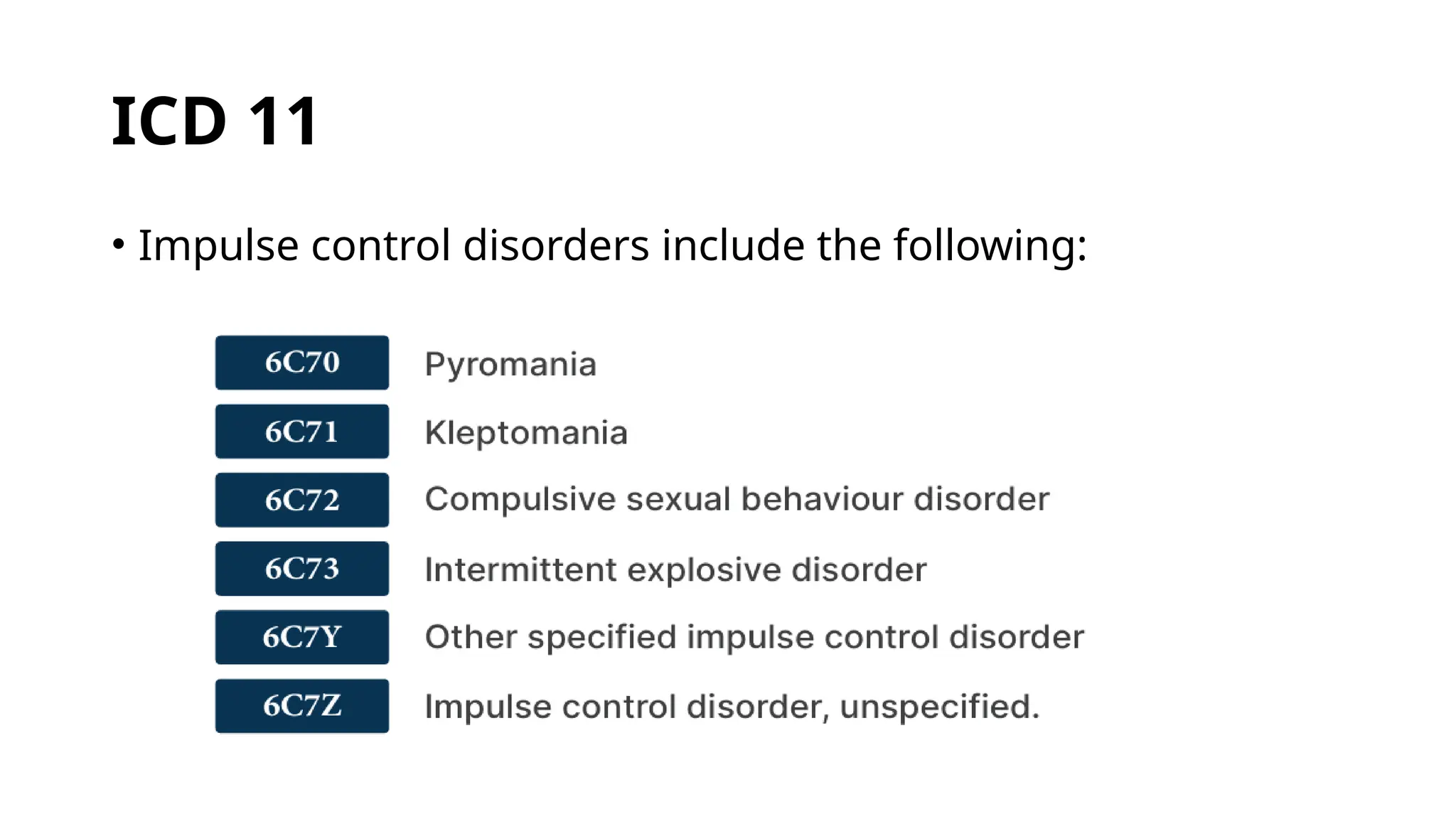
ICD 11
Trichotillomania-Working Group has recommended it to be
moved to the grouping of obsessive-compulsive and related
disorders in ICD-11
Skin picking (excoriation) disorder also be added with
Trichotillomania.
• Oppositional defiantdisorder (ODD)
• Intermittent explosive disorder (IED)
• Conduct disorder (CD)
• Kleptomania
• Pyromania
• The disorders mentioned above fall under disruptive, impulse-
control, and conduct disorders
17.
• Attention deficithyperactivity disorder (ADHD), trichotillomania, binge
eating disorder, and pathologic gambling disorders were removed and
relegated to neurodevelopmental, obsessive-compulsive, feeding, and
substance-related and addictive disorders, respectively
• DSM 5 now allows for ODD and CD to coexist phenomenologically and
offers a severity scale to be used in ODD
• Compulsive shopping and internet addiction now fall under 'other
specified disruptive, impulse control and conduct disorder.(Before they
belonged to a category known as disruptive behavior disorder (DBDNOS).
19.
Prevalence in generalpopulation
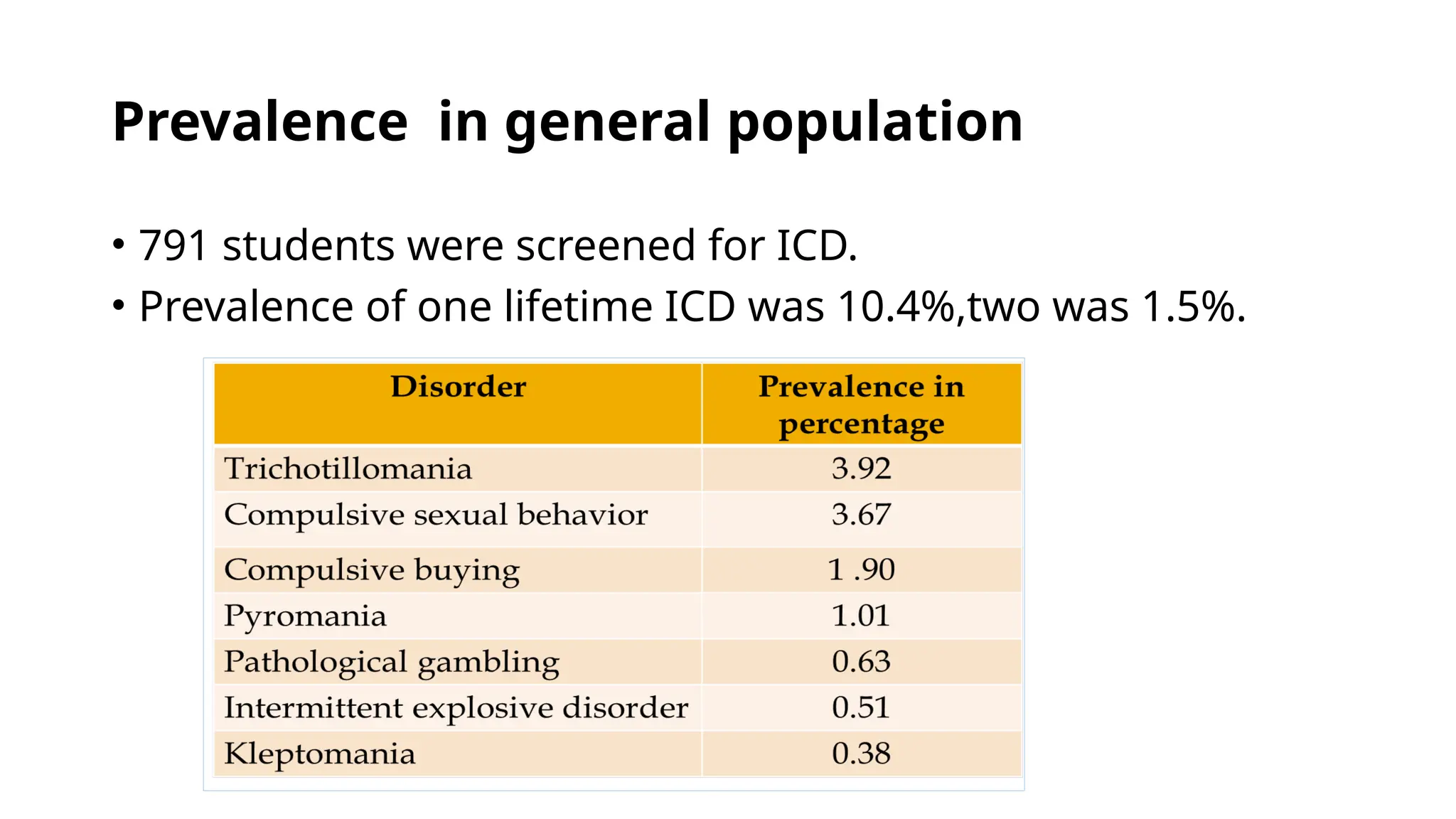
• 791 students were screened for ICD.
• Prevalence of one lifetime ICD was 10.4%,two was 1.5%.
20.
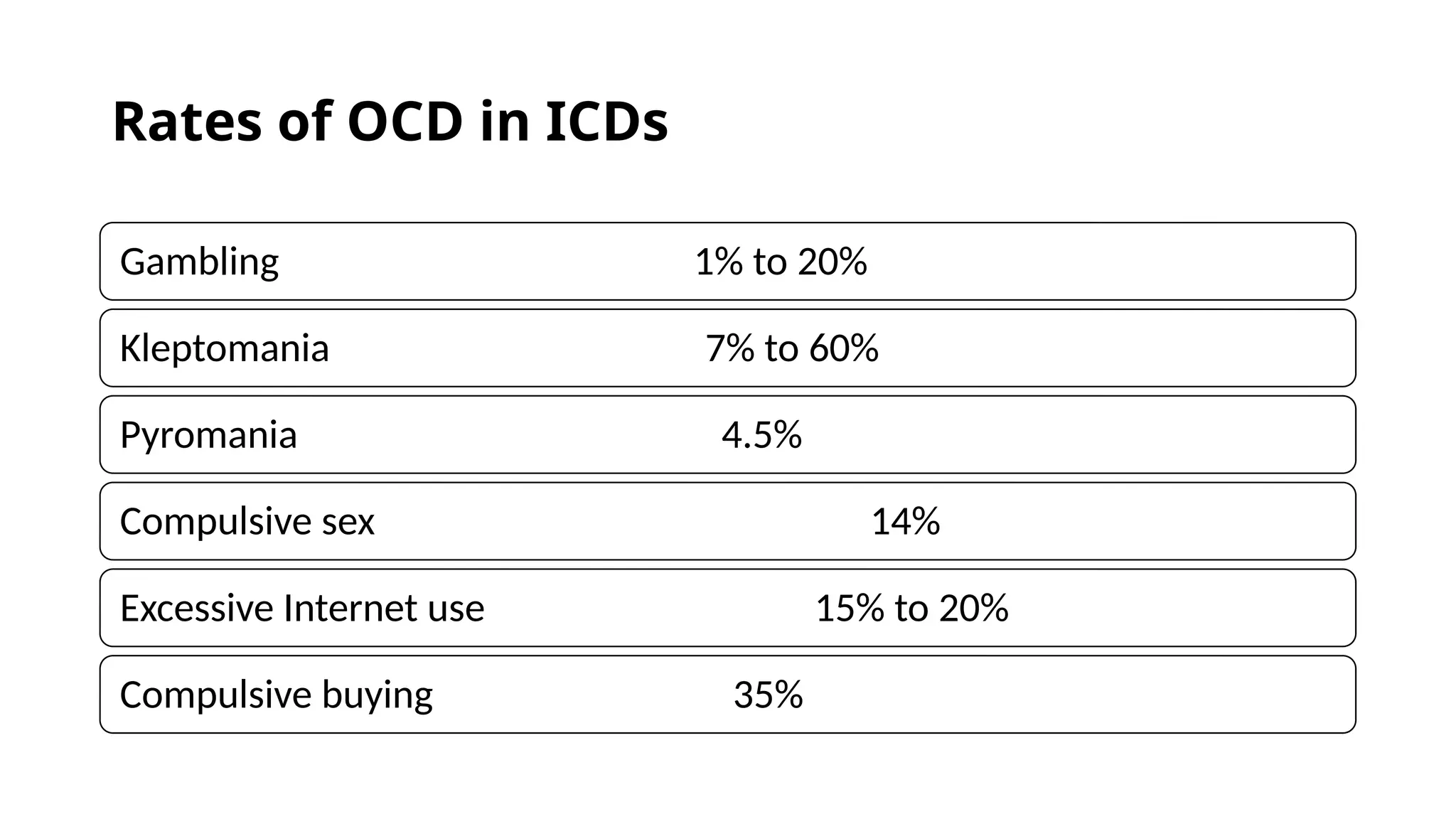
Rates of OCDin ICDs
Gambling 1% to 20%
Kleptomania 7% to 60%
Pyromania 4.5%
Compulsive sex 14%
Excessive Internet use 15% to 20%
Compulsive buying 35%
21.
ICD among Parkinson'sdisease
• Around 3000 PD patients interviewed for ICD
• More common in patients treated with a dopamine agonist than
in patients not taking a dopamine agonist [odds ratio:2.72]
23.
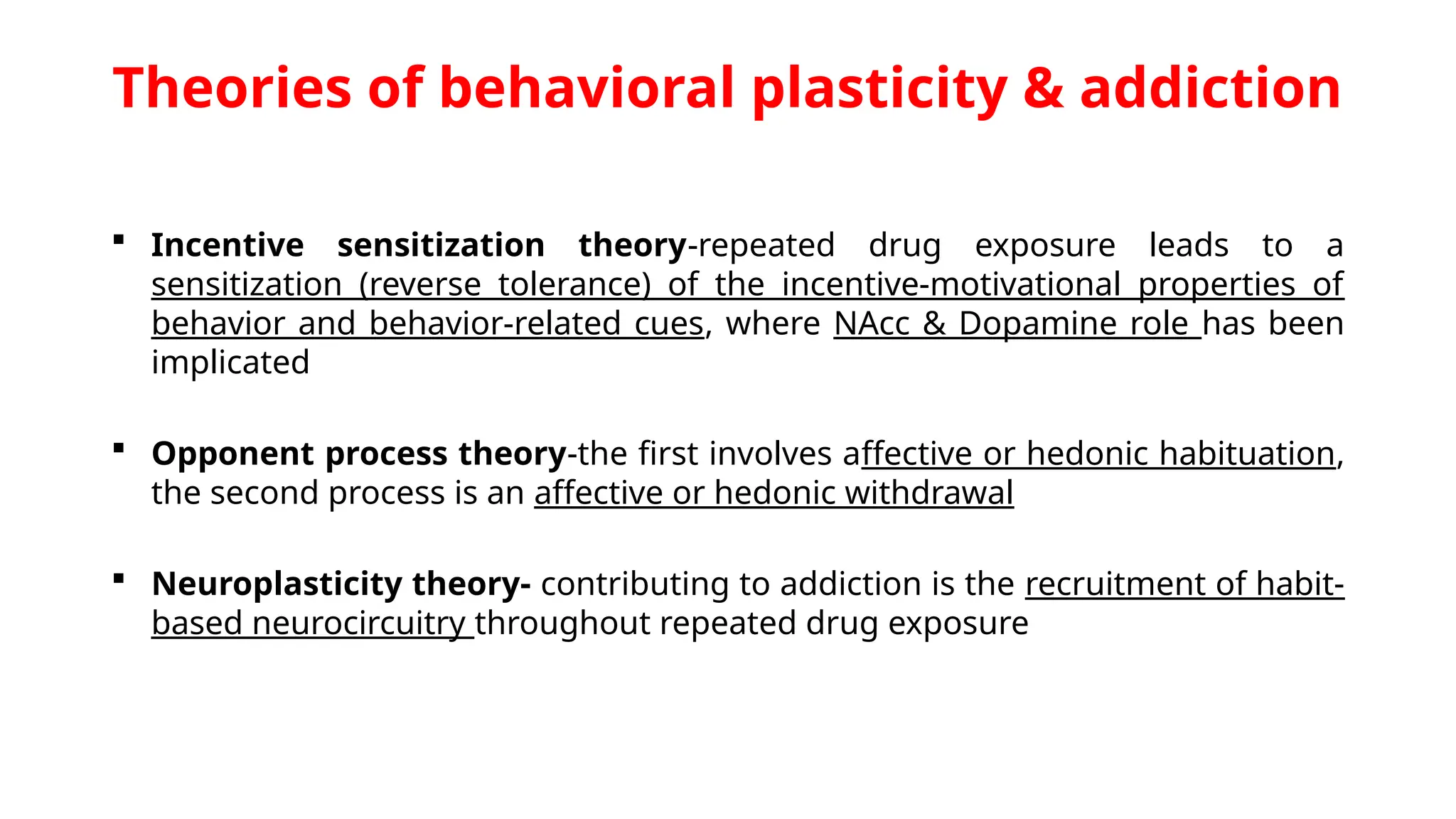
Theories of behavioralplasticity & addiction
Incentive sensitization theory-repeated drug exposure leads to a
sensitization (reverse tolerance) of the incentive-motivational properties of
behavior and behavior-related cues, where NAcc & Dopamine role has been
implicated
Opponent process theory-the first involves affective or hedonic habituation,
the second process is an affective or hedonic withdrawal
Neuroplasticity theory- contributing to addiction is the recruitment of habit-
based neurocircuitry throughout repeated drug exposure
24.
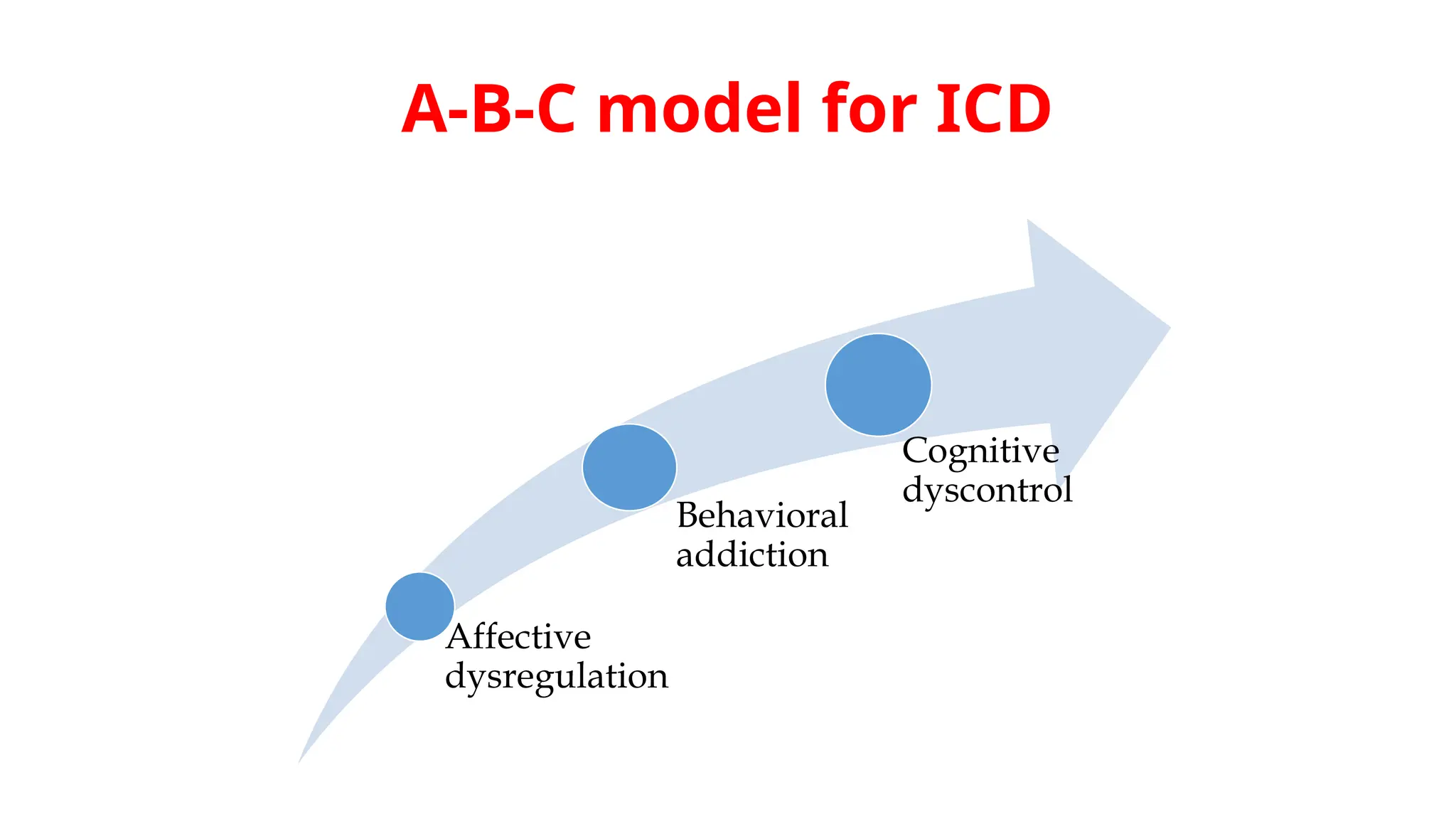
A-B-C model forICD
Affective
dysregulation
Behavioral
addiction
Cognitive
dyscontrol
INTERMITTENT EXPLOSIVE
DISORDER
• Intermittentexplosive disorder manifests as discrete
episodes of losing control of aggressive impulses; these
episodes can result in serious assault or the destruction of
property.
• The aggressiveness expressed is grossly out of proportion to
any stressors that may have helped elicit the episodes.
• The symptoms, which patients may describe as spells or
attacks, appear within minutes or hours and, regardless
of duration, remit spontaneously and quickly.
30.
Epidemiology
More common inmen than in
women.
More in first-degree biological
relatives of persons with the
disorder than in the general
population
Prevalence: rare
Course: variable; chronic or
episodic course
Onset: childhood to the early 20’s
Comorbidity
Higher association with
pyromania
Other disorders of impulse
control
substance use and mood, anxiety,
and eating disorders have also
been associated
31.
• ETIOLOGY
Psychodynamic Factors:
•Explosive outbursts occur as a defense against narcissistic
injurious events.
• Rage outbursts serve as interpersonal distance and protect
against any further narcissistic injury
Psychosocial Factors:
• Unfavorable childhood environment
• Early frustration, oppression, and hostility have been noted
as predisposing factors.
32.
Biological Factors
• Lowlevels of CSF 5-HIAA have been correlated with
impulsive aggression
• Decreased serotonergic transmission, decreases
the effect of punishment as a deterrent to behavior.
• High CSF testosterone correlated with
aggressiveness and violence in men
34.
DIFFERENTIAL DIAGNOSIS
• Conductdisorder:
repetitive & resistant pattern of behavior, as opposed to an episodic
pattern.
• Antisocial and borderline personality disorders:
Aggressiveness & impulsivity are part of patients' character & are
present between outbursts.
• Schizophrenia: patients show violent behavior in response to delusions
and hallucinations, and they show gross impairments in reality testing.
• Amok : It is an episode of acute violent behavior for which the person
claims amnesia. Amok is distinguished from intermittent explosive
disorder by a single episode and prominent dissociative features.
35.
COURSE AND PROGNOSIS
•It may begin at any stage of
life, but usually appears
between late adolescence and
early adulthood
• The disorder decreases in
severity with the onset of
middle age
36.
TREATMENT
• Group psychotherapy& family therapy
• Goal of therapy:
To have the patient recognize and verbalize
the thoughts or feelings that precede the
explosive outbursts instead of acting them
out.
• Anticonvulsants like carbamazepine,
valproate and phenytoin
• Selective serotonin reuptake inhibitors
(SSRIs)
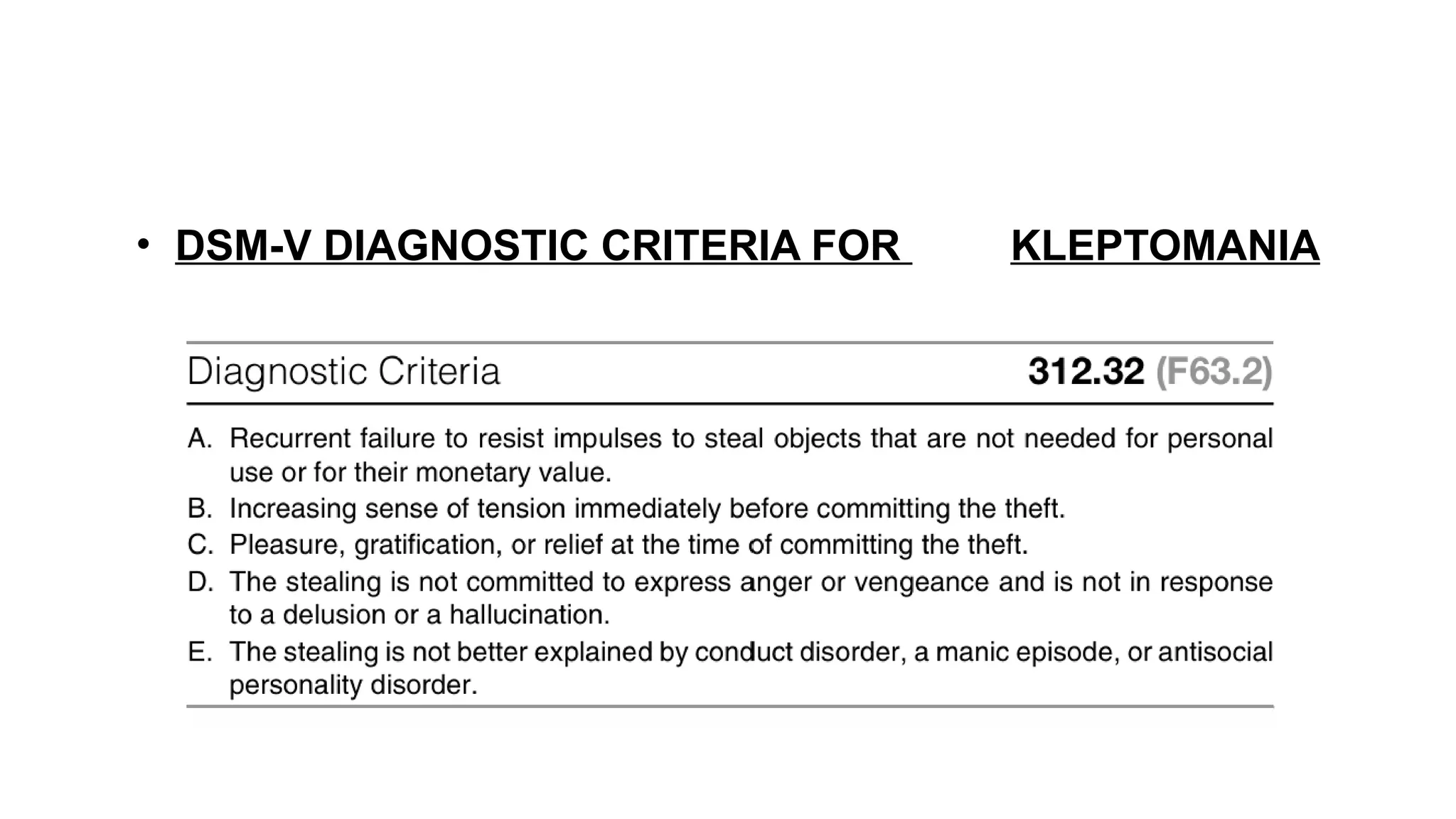
• KLEPTOMANIA
• Kleptomaniais the irresistible urge to steal items that you generally don't really need and
that usually have little value.
• The essential feature of kleptomania is a recurrent failure to resist impulses to steal
objects, not needed for personal use or for monetary value. The objects taken are often
given away, returned surreptitiously, or kept and hidden. Kleptomanics usually have the
money to pay for the objects they impulsively steal.
• It is crucial to differentiate kleptomania from common theft. In kleptomania, the patient
steals items that aren’t needed in terms of use and/or their financial value. The
shoplifting behavior is neither a response to anger or revenge nor triggered by
hallucinations or delusions. Similarly to other forms of impulse control disorders, patients
with kleptomania feel tensioned prior to performing the act of and relieved afterwards.
39.
EPIDEMIOLOGY
Prevalence estimated around0.6 %
Male-to-female ratio: 1:3
COMORBIDITY
• High lifetime comorbidity of affective disorder
(usually, but not exclusively, depression) and
various anxiety disorders.
• Other impulse-control disorders (notably,
pathological gambling and compulsive
shopping), eating & substance abuse disorders
40.
ETIOLOGY
• Anna Freudpointed out that the
first thefts from mother's purse
indicate the degree to which all
stealing is rooted.
• Karl Abraham wrote of the central
feeling of being neglected,
injured, or unwanted.
Self help books for
psychology
41.
• One theoreticianestablished 7 categories of stealing in chronically
acting-out children:
1) As a means of restoring the lost mother child relationship
2) As an aggressive act
3) As a defense against fears of being damaged (perhaps a search by
girls for a penis or a protection against castration anxiety in boys)
4) As a means of seeking punishment
5) As a means of restoring or adding to self-esteem
6) In connection with, and as a reaction to, a family secret
7) As excitement (lust angst) and a substitute for a sexual act
• One or more of these can also apply to adult kleptomania
ICD – 10PATHOLOGICAL STEALING
(KLEPTOMANIA)
• There are two or more thefts in
which the individual steals without
any apparent motive of personal
gain or gain for another person.
• The individual describes an
intense urge to steal, with a
feeling of tension before the act
and relief afterward
44.
COURSE AND PROGNOSIS
•Onset : late adolescence.
• Mean age
Men : 50 yrs & Women : 35 yrs
• Course: waxes & wanes, but tends
to be chronic
• Prognosis with treatment can be
good, but few patients come for
help
45.
TREATMENT
• Behavior therapy,including
systematic desensitization,
aversive conditioning
• SSRIs, such as fluoxetine &
fluvoxamine, appear to be
effective in some patients
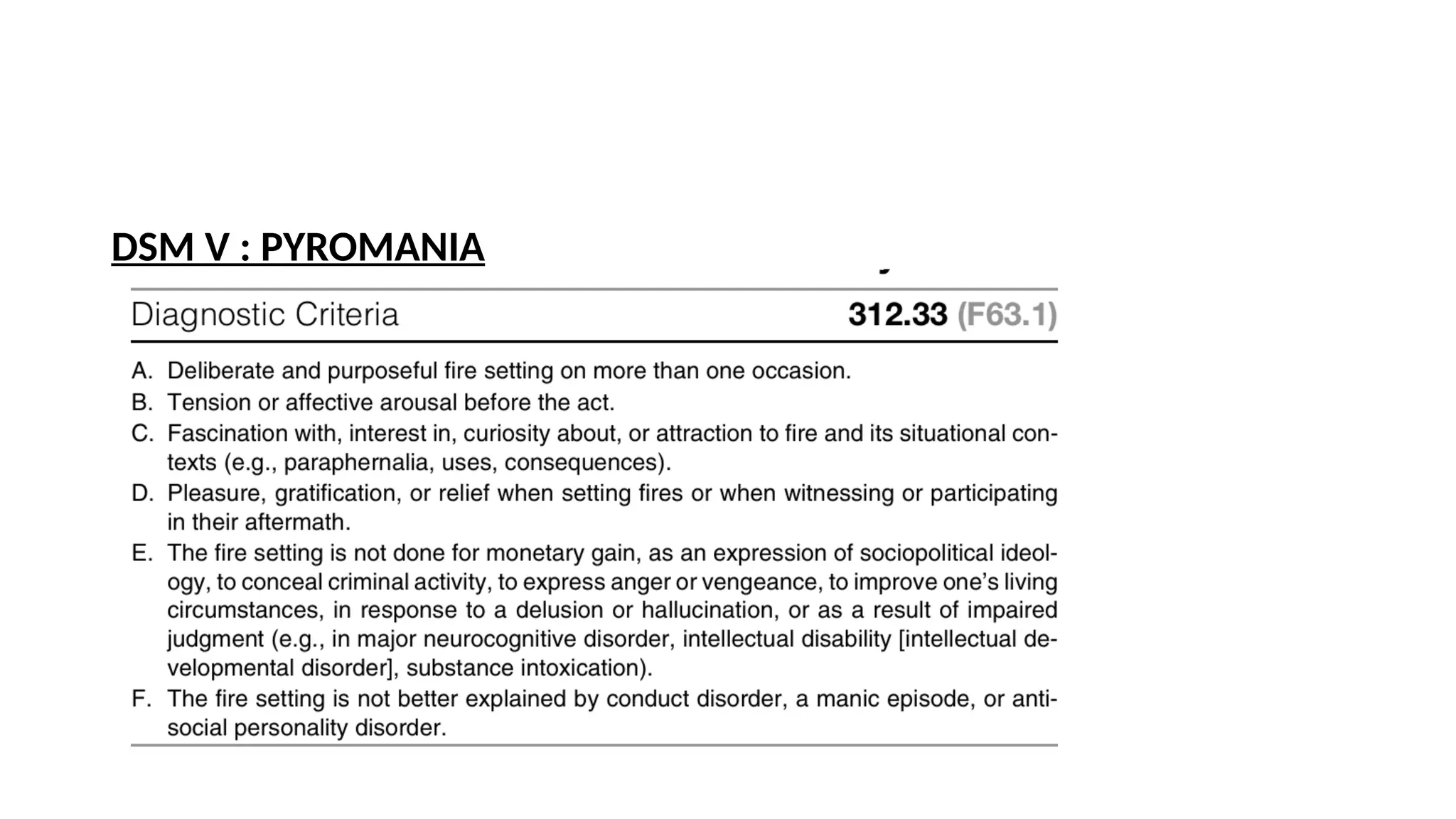
PYROMANIA
• Pyromania isthe recurrent, deliberate, and purposeful setting of fires.
Associated features include tension or affective arousal before setting the
fires; fascination with, interest in, curiosity about, or attraction to fire and
the activities and equipment associated with firefighting; and pleasure,
gratification, or relief when setting fires or when witnessing or participating
in their aftermath.
• The diagnosis of pyromania necessitates the occurrence of more than one
occasion during which the patient attempts deliberately setting fire.
Moreover, the patient usually feels stressed before setting the fire and
relieved after performing the act.
• Pyromania is extremely rare and literature data is rather scarce
48.
EPIDEMIOLOGY
• Prevalence :unknown
• Male to female ratio : 8 to 1
COMORBIDITY
• Substance abuse disorder & affective disorders;
• Other impulse control disorders, such as kleptomania in female fire setters;
• Personality disturbances, such as antisocial & borderline personality disorders.
• Attention-deficit disorder and learning disabilities may be associated with
childhood pyromania;
• Persons who set fires are more likely to be mildly retarded than are those in
the general population.
49.
ETIOLOGY
Psychosocial
• Freud sawfire as a symbol of sexuality.
• He believed the warmth radiated by fire evokes the same sensation that
accompanies a state of sexual excitation, and a flame's shape and movements
suggest a phallus in activity.
• Some patients with pyromania are volunteer firefighters who set fires to prove
themselves brave, to force other firefighters into action, or to demonstrate their
power to extinguish a blaze.
• The act is a way to vent accumulated rage over frustration caused by a sense of
social, physical, or sexual inferiority.
50.
• Several studieshave noted that the fathers of patients with pyromania
were absent from the home.
• One explanation of fire setting is that it represents a wish for the
absent father to return home as a rescuer, to put out the fire, and to
save the child from a difficult existence.
Biological Factors
• Low CSF levels of 5-HIAA and 3-methoxy-4-hydroxyphenylglycol
(MHPG) - It suggests possible serotonergic or adrenergic involvement.
• ICD –10 PYROMANIA
• There are two or more acts of fire setting without apparent
motive.
• The individual describes an intense urge to set fire to objects,
with a feeling of tension before the act and relief afterward.
• The individual is preoccupied with thoughts or mental images of
fire setting or of the circumstances surrounding the act (e.g.,
abnormal interest in fire engines or in calling out the fire service
53.
COURSE AND PROGNOSIS
•Begins in childhood, the typical age of onset is unknown.
• When onset is in adolescence or adulthood, the fire setting tends to
be deliberately destructive.
• It is episodic & may wax & wane in frequency.
• Prognosis for treated children is good, and complete remission is a
realistic goal.
• Prognosis for adults is guarded, because they frequently deny their
actions, refuse to take responsibility, are dependent on alcohol, &
lack insight
54.
TREATMENT
• Treatment difficultbecause of their lack of motivation.
• No single treatment has been proved effective; thus a number
of modalities, including behavioral approaches, should be tried.
• Because of the recurrent nature, any treatment program should
include supervision of patients to prevent a repeated episode of
fire setting.
• In children and adolescents, treatment should include family
therapy
55.
Conclusion
• Relationship betweenImpulsivity & compulsivity are intricate. These
symptoms overlap in many psychiatric disorders
• Limited studies on epidemiology at present. There exists tremendous
scope for research in this direction
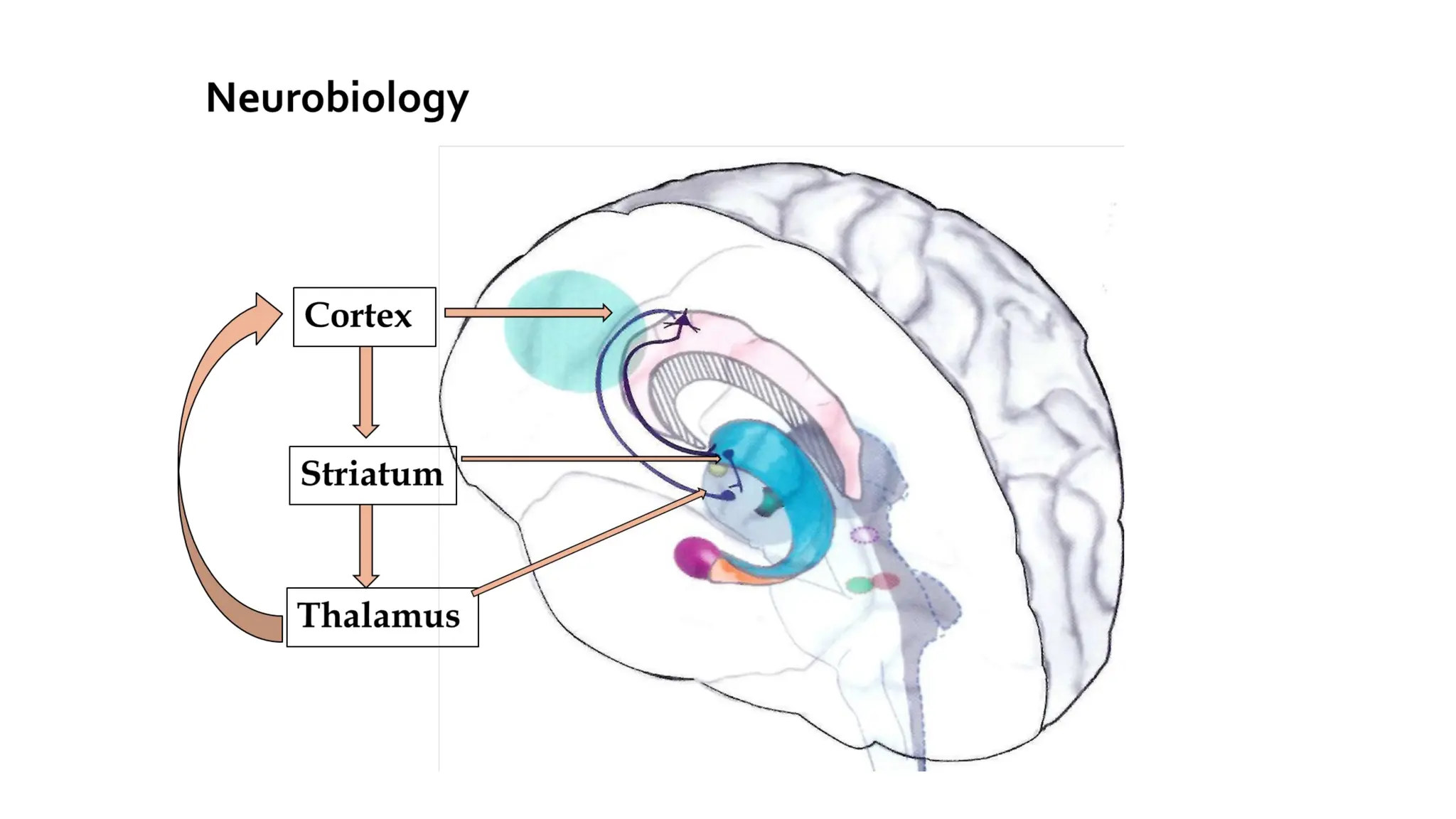
• Evidence in neurobiology shows involvement of reward pathway including
vmPFC, OFC, Striatum[ventral to dorsum] in all ICD similar to substance use
disorder
56.
• TTM, skinpicking resemble OC related disorders, but Pathological
gambling, other newer additions like compulsive sexual behavior,
compulsive buying, internet addiction, food addiction, exercise addiction
resemble substance use disorder- reflecting the progress in understanding
of these conditions.
• Proposed changes in ICD 11 and DSM 5 reflects the better understanding
and progress in research among these conditions
57.
• To includeIED by DSM 5 - in disruptive, impulse & conduct
disorder
• Pathological gambling by DSM 5- in ‘Substance & Addictive
Disorder.’
• Newer Behavioral Addictions need more time and work to understand,
conduct epidemiological studies and only then consider them in the
classificatory system, hence tremendous potential for research in this area.
58.
References
• Moeller FG,Barratt ES, Dougherty DM, Schmitz JM, Swann AC. Psychiatric aspects of impulsivity. Am
J Psychiatry. 2001 Nov;158(11):1783-93. doi: 10.1176/appi.ajp.158.11.1783. PMID: 11691682.
• Jon E. Grant, Stephen Correia, Thea Brennan-Krohn,White matter integrity in kleptomania: A pilot
study,Psychiatry Research: Neuroimaging,Volume 147, Issues 2–3,2006,Pages 233-237,ISSN 0925-
4927,https://doi.org/10.1016/j.pscychresns.2006.03.003.
• Fineberg NA, Potenza MN, Chamberlain SR, Berlin HA, Menzies L, Bechara A, Sahakian BJ, Robbins
TW, Bullmore ET, Hollander E. Probing compulsive and impulsive behaviors, from animal models to
endophenotypes: a narrative review. Neuropsychopharmacology. 2010 Feb;35(3):591-604. doi:
10.1038/npp.2009.185. Epub 2009 Nov 25. PMID: 19940844; PMCID: PMC3055606.
• Kaplan & sadock's synopsis of psychiatry behavioural sciences/clinical psychiatry 11th
edition
• Hollander, E., & Benzaquen, S. D. (1997). The obsessive-compulsive spectrum disorders. International
Review of Psychiatry, 9(1), 99-110. https://doi.org/10.1080/09540269775628
59.
• Olsen CM.Natural rewards, neuroplasticity, and non-drug addictions. Neuropharmacology. 2011
Dec;61(7):1109-22. doi: 10.1016/j.neuropharm.2011.03.010. Epub 2011 Apr 1. PMID: 21459101; PMCID:
PMC3139704.
• Natalie L. Cuzen, Dan J. Stein,Chapter 2 - Behavioral Addiction: The Nexus of Impulsivity and
Compulsivity,Editor(s): Kenneth Paul Rosenberg, Laura Curtiss Feder,Behavioral Addictions,Academic
Press,2014,Pages 19-34,ISBN 9780124077249,https://doi.org/10.1016/B978-0-12-407724-9.00002-1.
• Brewer JA, Potenza MN. The neurobiology and genetics of impulse control disorders: relationships to
drug addictions. Biochem Pharmacol. 2008 Jan 1;75(1):63-75. doi: 10.1016/j.bcp.2007.06.043. Epub 2007 Jul
3. PMID: 17719013; PMCID: PMC2222549.
• Diagnostic and statistical manual of mental disorders fifth edition text revision dsm-5
• Grant JE, Odlaug BL, Kim SW. Kleptomania: clinical characteristics and relationship to substance use
disorders. Am J Drug Alcohol Abuse. 2010 Sep;36(5):291-5. doi: 10.3109/00952991003721100. PMID:
20575650.
• Weintraub D, Koester J, Potenza MN, Siderowf AD, Stacy M, Voon V, Whetteckey J, Wunderlich GR, Lang AE.
Impulse control disorders in Parkinson disease: a cross-sectional study of 3090 patients. Arch Neurol.
2010 May;67(5):589-95. doi: 10.1001/archneurol.2010.65. PMID: 20457959.
• Sadock BJ, Sadock VA, Pedro Ruiz. Comprehensive Textbook of Psychiatry 10th
ed. 2017 Wolters Kluwer
#4 Definition: Impulsivity refers to rapid and unplanned reactions to stimuli that occur before an individual has fully processed the information. This behavior is characterized by several key features:
Immediate Reactions:
Individuals often respond quickly to stimuli, without taking the time to think through their actions or the potential outcomes. This can lead to hasty decisions.
Decreased Sensitivity to Negative Consequences:
Those who are impulsive tend to show reduced awareness of the negative consequences of their behaviors. They may engage in risky activities without fully considering the repercussions.
Neglect of Long-Term Consequences:
Impulsive individuals often focus on immediate rewards or gratification, lacking consideration for how their actions may impact them or others in the long run.
Impact on Others:
Impulsivity does not only affect the individual exhibiting these behaviors; it can also significantly impact friends, family, and broader social circles, leading to relational or situational conflicts.
Failure to Inhibit Reward-Motivated Behaviors:
There is a tendency for individuals to struggle with inhibiting behaviors driven by immediate rewards, leading to further impulsive actions.
#6 Repetitive Behaviors:
Definition: These are actions performed repeatedly, often as a means to alleviate tension or to cope with negative emotional states.
Key Feature: Individuals may struggle to suppress these behaviors despite recognizing that they are not productive or beneficial. This inability to control such actions can exacerbate feelings of distress or anxiety.
Reference: Grant et al. (2006) highlight the connection between these repetitive behaviors and the underlying need to relieve tension or negative emotions.
Desire to Avoid Harm:
Definition: This refers to an inherent drive to evade situations or actions that could lead to physical or emotional harm.
Key Feature: The motivation to avoid harm can significantly influence behavior, often leading individuals to engage in repetitive actions as a maladaptive coping mechanism.
#7
Here's a concise overview based on the provided statements regarding the concept of a spectrum in mental health disorders:
Spectrum of Mental Health Disorders
Conceptual Framework:
Mental health disorders are not a unitary disorder but rather a syndrome composed of subgroups. This perspective acknowledges the complexity and diversity within mental health conditions.
Linked Conditions:
There exists a range of linked conditions that share common features or underlying mechanisms. This connection can help clinicians and researchers better understand and treat these disorders.
Spectrum Characteristics:
Similar Appearance: The different elements within these spectra often present with similar symptoms or characteristics, making it challenging to categorize them distinctly.
Underlying Mechanisms: Many of these conditions are believed to stem from the same underlying mechanisms, whether biological, psychological, or environmental.
Examples of Spectra:
Bipolar Spectrum: Encompasses a range of mood disorders that share characteristics related to mood fluctuations, including bipolar I, bipolar II, and cyclothymic disorder.
Schizophrenia Spectrum: Includes schizophrenia and related disorders, highlighting the continuum of psychotic symptoms and varying levels of functional impairment.
Obsessive-Compulsive Spectrum: Comprises obsessive-compulsive disorder (OCD) and related conditions, emphasizing the shared compulsive and obsessive features across this group.
#8 Figure 1. The overview of obsessive compulsive spectrum disorders*. Abbreviations: AN anorexia nervosa, ASPD antisocial personality disorder, Aut autism, BDD body dysmorphic disorder, BPD borderline personality disorder, Del OCD delusional OCD, Dep depersonalization disorder, Ep epilepsy, Hun Huntington’s disease, Hyp hypochondriasis, Klep kleptomania, ObSc obsessional schizophrenia, PD personality disorder, PG pathological gambling,ScOCD schizotypalOCD,Sexcomp sexual compulsions,SIB self-injuriousbehaviour, Syd Sydenham’schorea,Trich trichotillomania,TS Tourette’ssyndrome.(ReprintedwithpermissionfromHollander,
#19 The screening of 791 students for Impulse Control Disorders (ICD) revealed the following prevalence rates:
One lifetime ICD: 10.4% (which means about 82 students)
Two lifetime ICDs: 1.5% (approximately 12 students)
#23 Repeated drug exposure increases sensitivity (reverse tolerance) to the incentive-motivational properties of drugs.
This means the brain becomes more responsive to drug-related cues over time, increasing the urge to seek the drug.
Role of dopamine and nucleus accumbens (NAcc): Dopamine spikes in response to cues associated with drug use, driving the desire for the drug.
The NAcc and dopamine pathways play a key role in the brain’s reward system.Over time, these pathways become hypersensitive to drug-related stimuli.This sensitization leads to an increased craving or "wanting" of the drug, even if the pleasure or "liking" decreases.Reason: Incentive sensitization explains why addicts develop strong cravings even when the pleasurable effects of the drug diminish over time.
Addiction involves two processes:The A-process: an initial pleasurable response (hedonic or affective).
The B-process: a withdrawal response that kicks in as the pleasurable effects fade.
Over time, the B-process grows stronger, resulting in affective withdrawal after drug use.Users take the drug not just for pleasure, but to avoid negative feelings during withdrawal.
Affective habituation: With repeated drug use, the pleasurable effects (A-process) weaken.Affective withdrawal: The B-process (withdrawal symptoms) intensifies, motivating continued drug use to avoid discomfort.Reason: The theory explains the development of physical dependence and why addicts continue drug use to avoid negative emotions, even when they no longer experience strong positive effects.
Neuroplasticity refers to the brain's ability to change and adapt in response to experience.Repeated drug use leads to long-lasting changes in the brain’s structure and function, especially in circuits related to habit formation.These changes recruit habit-based neurocircuitry in areas like the basal ganglia, making drug-seeking behavior habitual and automatic.
Drug use shifts from goal-directed behavior (initially driven by pleasure) to habitual behavior, controlled by different brain regions.Basal ganglia and prefrontal cortex undergo neuroplastic changes, reinforcing habitual drug-seeking and reducing impulse control.Reason: This theory explains why addiction is difficult to break, as repeated drug exposure hardwires the brain into habitual patterns that override rational decision-making.
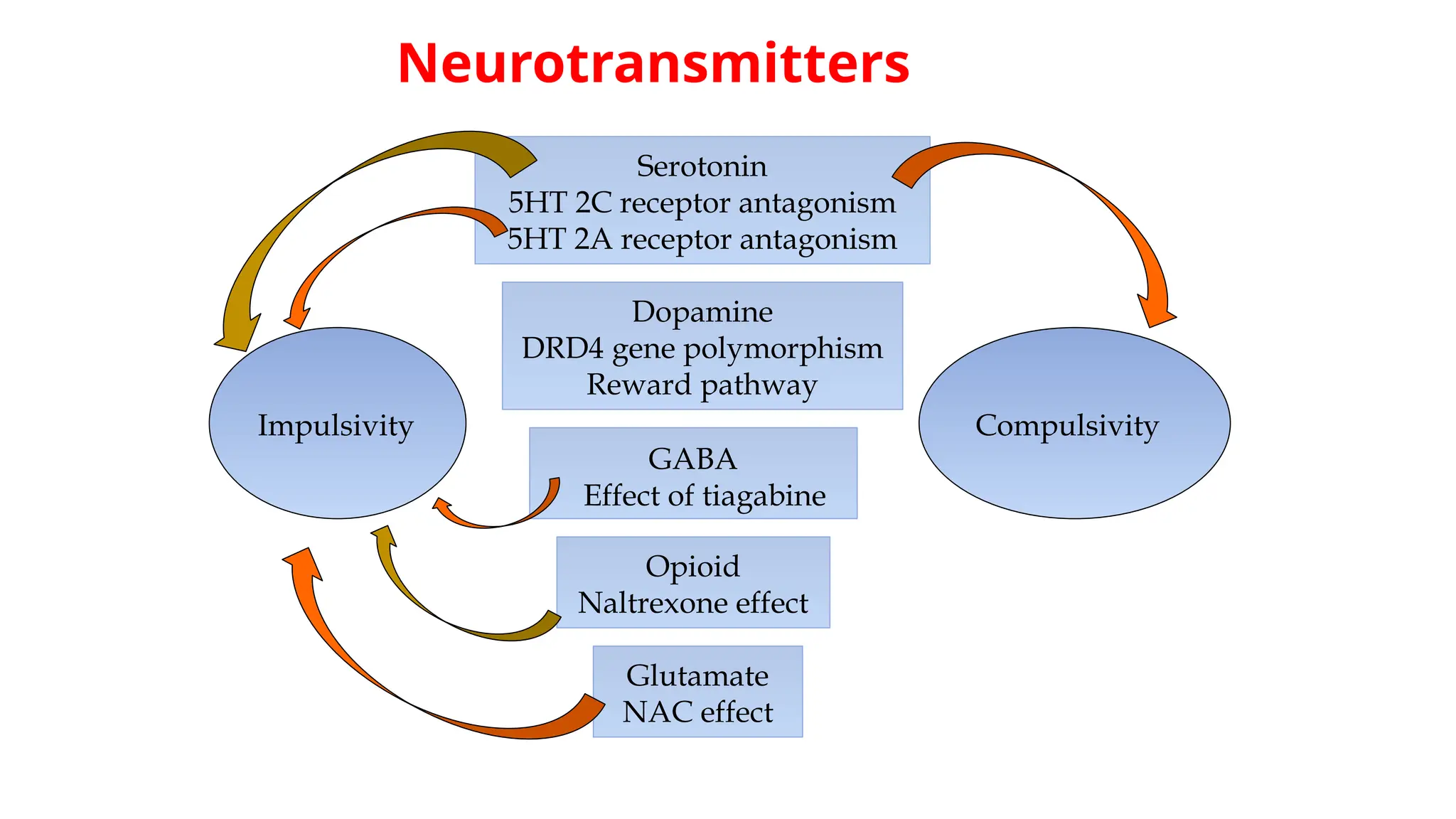
#24 The relationship between negative affect (emotions like sadness, stress, or anxiety) and compulsive-impulsive behavior, including substance addiction. Several studies suggest that negative emotions play a key role in triggering both compulsive behavior and substance abuse. This aligns with research showing that negative affect is closely tied to addiction during both the initial stages of use and its continuation
Compulsive-impulsive behaviors share neurobiological pathways with substance addiction, involving serotonin and dopamine system alterations. Impaired impulse control and reward sensitivity are key factors. Neuroimaging shows that brain regions activated by addiction are also linked to compulsive behaviors. While no specific medications exist for these behaviors, drugs like **naltrexone** and **topiramate**, used for addiction, have shown promise in treating compulsive-impulsive behaviors by targeting similar pathways.
Impulsivity is a key feature of both substance addiction and compulsive-impulsive behaviors, often due to dysregulation of prefrontal cortex circuitry and altered glutamate and dopamine function. This impairs inhibitory control, increasing impulsivity. To combat this, psychosocial treatments aim to strengthen cognitive control through relapse prevention strategies, which focus on identifying abuse patterns, managing high-risk situations, and adopting healthier behaviors. Effective therapies include motivational enhancement, cognitive-behavioral therapy (CBT), and 12-step programs, which have been successful in treating compulsive behaviors like gambling, kleptomania, and compulsive buying.
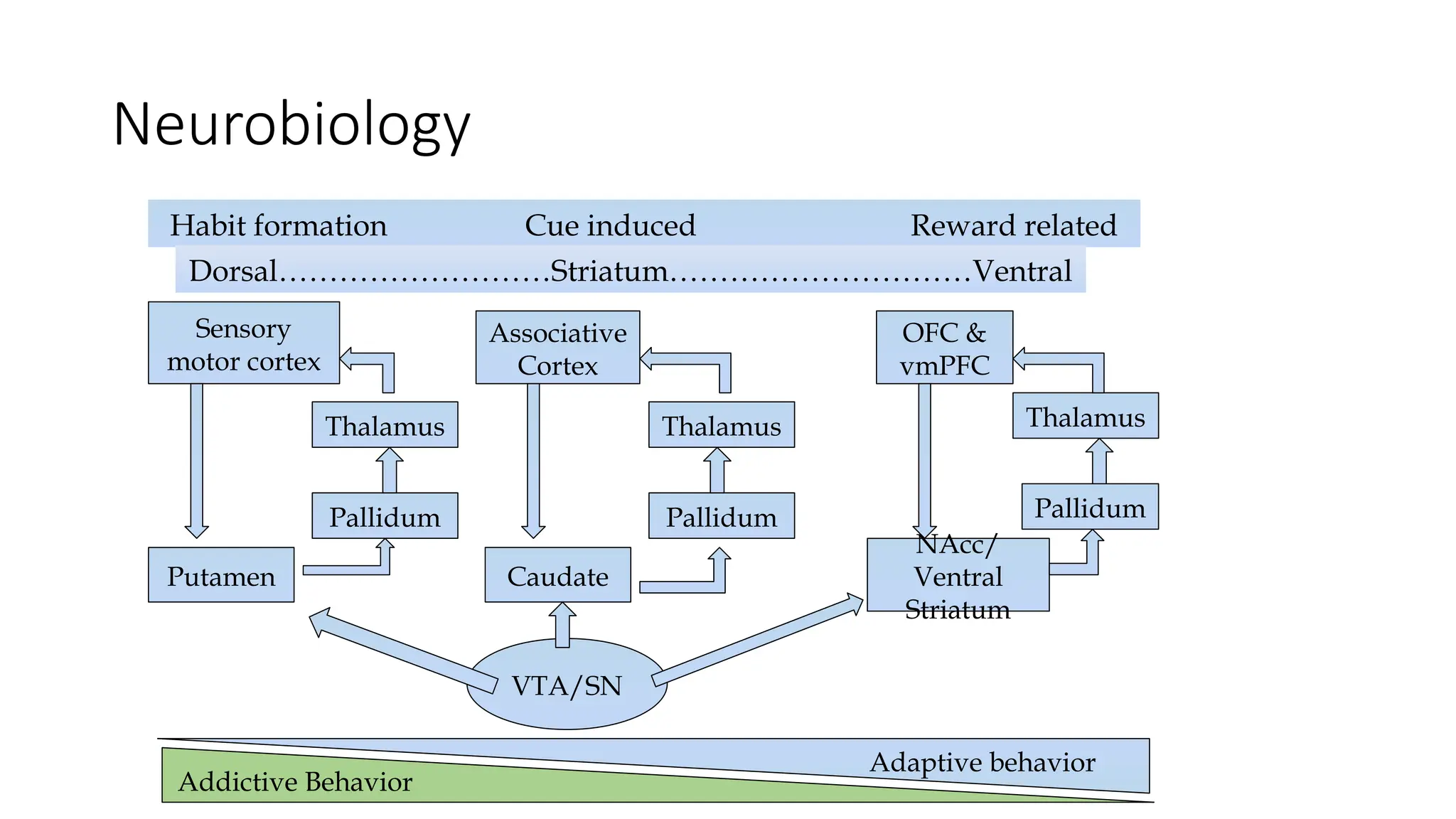
#25 Prefrontal Cortex (PFC):
The PFC, especially the ventromedial PFC (vmPFC) and orbitofrontal cortex (OFC), plays a crucial role in decision-making, impulse regulation, and self-control.
In ICDs, hypofunction of the PFC leads to poor inhibitory control, reducing the ability to suppress impulses.
Striatum (Dorsal & Ventral):
The ventral striatum, including the nucleus accumbens (NAcc), is involved in reward processing.
In ICDs, the striatum becomes hyperactive, leading to increased sensitivity to rewards or cues related to the impulsive behavior.
Amygdala:
Involved in emotional processing and regulating responses to reward and punishment.
Dysfunction in the amygdala can heighten emotional reactivity and drive impulsive behavior in response to stress or emotional triggers.
#30 Definition: The cycle of violence refers to a pattern often observed in abusive relationships, characterized by a repeating cycle of tension building, explosive incidents of violence, and periods of reconciliation or calm. This cycle can perpetuate and normalize violent behavior within relationships and families.
Phases:
Tension-Building Phase: Stress and conflict escalate, leading to increased anxiety and irritability.
Explosive Phase: An aggressive incident occurs, often in the form of physical or verbal abuse.
Honeymoon Phase: After the explosion, there may be a temporary period of calm, during which the abuser may apologize or show remorse.
Link Between IED and the Cycle of Violence
Aggressive Behavior: Individuals with IED may exhibit behaviors that align with the explosive phase of the cycle of violence, demonstrating an inability to manage their anger and impulsivity. Their aggressive outbursts can contribute to a cycle of violence in relationships or family dynamics.
Family History of Violence: Research suggests that individuals with IED often have a history of exposure to violence, whether through family environments or personal experiences. This exposure can contribute to the normalization of aggression and the perpetuation of violent behaviors across generations.
Emotional Dysregulation: Both IED and the cycle of violence are characterized by emotional dysregulation, where individuals struggle to control their emotions and reactions. This dysregulation can lead to repeated cycles of violence in personal relationships, creating a toxic environment.
Potential for Escalation: The impulsivity seen in IED may escalate situations rapidly, increasing the frequency and severity of violent incidents in the cycle of violence. As the pattern continues, it can lead to more serious forms of aggression and harm.
#31 1. Psychodynamic Factors:
Defense Mechanism Against Narcissistic Injury:
Explosive outbursts are seen as a way to defend the self against narcissistic injuries (emotional wounds to self-esteem).
The intense emotional response acts as a protective mechanism to avoid feeling vulnerable or further emotionally wounded.
Rage as a Defense Strategy:
Rage outbursts create interpersonal distance, pushing others away and protecting the individual from deeper emotional pain or further threats to their ego.
These outbursts serve to restore a sense of control and preserve self-image when the individual feels their self-worth is under attack.
2. Psychosocial Factors:
Unfavorable Childhood Environment:
Individuals with impulse control disorders often have a history of a dysfunctional upbringing, where they lacked appropriate emotional support.
Early Frustration, Oppression, and Hostility:
Childhood adversity, including frustration, oppression, and exposure to hostility, is a significant predisposing factor.
These early experiences may result in maladaptive coping mechanisms, where impulsive or explosive behaviors become a way to express unresolved emotional tension and frustration.
#32 Low Levels of CSF 5-HIAA and Impulsive Aggression:
5-HIAA (5-hydroxyindoleacetic acid) is a metabolite of serotonin. Low levels of 5-HIAA in cerebrospinal fluid (CSF) have been linked to impulsive aggression.
Reduced serotonin levels impair emotional regulation, making it more difficult to control aggressive impulses.
Serotonergic dysregulation is a key factor in increasing impulsivity and aggression in individuals with impulse control disorders.
Decreased Serotonergic Transmission:
Decreased serotonin activity diminishes the brain’s response to punishment as a deterrent to negative behavior.
This lack of response to punishment allows individuals to engage in impulsive behaviors without feeling the usual consequences (guilt, fear of punishment), contributing to behavioral disinhibition.
Impulsivity is often the result of serotonin deficiency, which leads to poor impulse control and a reduced capacity to learn from negative experiences.
High CSF Testosterone Levels and Aggression:
Elevated testosterone levels in the CSF have been correlated with increased aggression and violence, particularly in men.
Testosterone is linked to increased dominance and risk-taking behaviors, which may lead to more impulsive actions.
High testosterone levels can also heighten sensitivity to provocation, increasing the likelihood of aggressive responses.
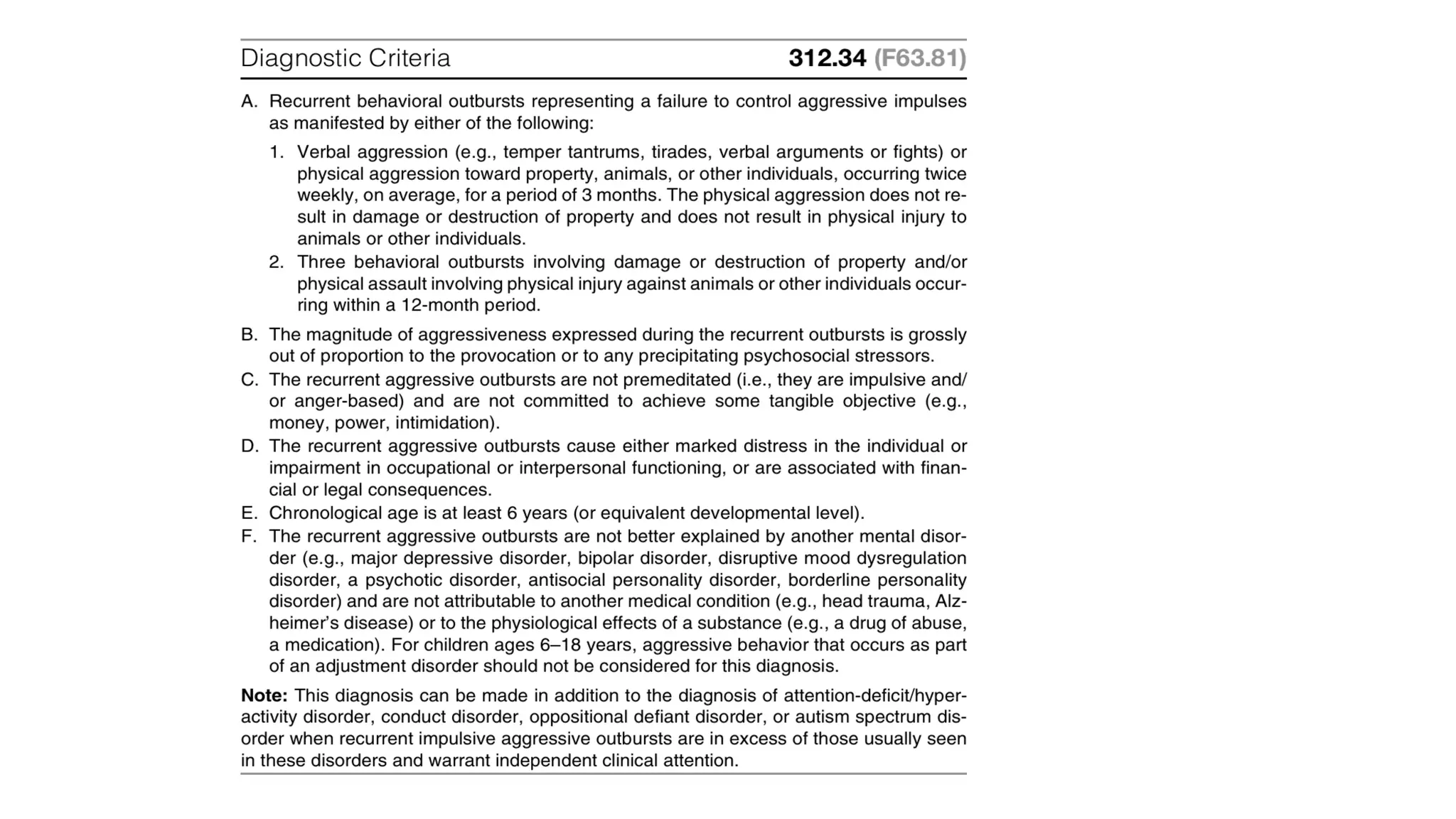
#33 Impulsive and Anger-Based Aggressive Outbursts:
Outbursts have a rapid onset, typically with no prodromal period (i.e., no noticeable warning signs beforehand).
These outbursts often last for less than 30 minutes and usually occur in response to minor provocations, such as trivial incidents or arguments, often with close associates or intimate partners.
Two Types of Aggressive Episodes:
Frequent, less severe outbursts (Criterion A1):
Occur twice weekly on average over a 3-month period.
These involve verbal aggression (e.g., temper tantrums, verbal arguments) or nondamaging physical aggression (e.g., minor physical fights).
No significant destruction of property or injury is involved in these episodes.
Infrequent, more severe outbursts (Criterion A2):
Occur at least three times in a year.
These involve significant damage to objects (regardless of value) or physical assaults that cause injury to people or animals.
Core Feature: Failure to Control Aggressive Impulses (Criterion B):
The individual is unable to control their aggressive behavior when faced with a subjectively experienced provocation that would not normally result in an outburst for most people.
Outbursts are generally impulsive (i.e., not premeditated) and arise due to emotional dysregulation, rather than being calculated or instrumental (Criterion C).
#36 Individual psychotherapies
Group psychotherapies
Anger management
Medications used in the treatment of IEDs are all off –label!
Examples include:
Mood stabilizers such as Lithium and the anticonvulsants
Beta blockers
SSRIs
#38 Here’s a shortened version of the table for speaker notes:
| **Aspect** | **Kleptomania** | **Pathological Stealing** |
|--------------------------|------------------------------------------|--------------------------------------------|
| **Motivation** | Impulsive urge to steal. | External reasons like financial gain. |
| **Planning** | Unplanned, compulsive. | Often planned and goal-oriented. |
| **Emotional Experience** | Tension before, relief after; guilt. | Less emotional involvement; no guilt. |
| **Use of Items** | Discards or hides stolen items. | Uses or sells stolen items. |
| **Classification** | Impulse control disorder. | Not a mental health disorder. |
| **Co-occurring Issues** | Linked to anxiety, depression, OCD. | Linked to conduct or antisocial disorders. |
#40 Anna Freud's Perspective:
Developmental Insight: Anna Freud, a key figure in psychoanalytic theory, posited that early childhood experiences profoundly shape personality and behavior. In her view, initial thefts from a caregiver's purse, especially from a mother, signify deeper emotional issues. These early acts of stealing may stem from a child’s desire for attention, control, or autonomy in a relationship that might feel overwhelming or unresponsive.
Rooted in Attachment: Freud emphasized the importance of attachment in child development. If a child feels neglected or experiences inconsistent responses from their caregiver, they might engage in stealing as a maladaptive strategy to cope with feelings of abandonment or inadequacy. Such early thefts could represent an unconscious attempt to gain the caregiver's attention or to express unfulfilled emotional needs.
Behavior as Communication: For children, stealing can serve as a form of communication regarding their emotional state. It reflects an internal struggle with feelings of worthlessness, and the act of theft may momentarily alleviate emotional distress or provide a sense of power.
Karl Abraham's Perspective:
Neglect and Injury: Karl Abraham built on Freudian concepts by highlighting the psychological effects of feeling neglected or unwanted during formative years. According to Abraham, individuals who experience chronic feelings of neglect or emotional injury are at risk for developing maladaptive behaviors, including kleptomania. These feelings may arise from various factors, such as parental indifference, emotional abuse, or inadequate support during critical developmental stages.
Emotional Deficits: Abraham posited that the central emotional experience of feeling unwanted can lead to a compensatory need for validation or self-worth. For some, stealing might serve as a misguided attempt to fill an emotional void, creating a temporary sense of satisfaction or fulfillment.
Psychological Mechanism: The compulsion to steal can be viewed as a defense mechanism against feelings of worthlessness. The act of theft provides a fleeting sense of control and empowerment, temporarily masking deeper emotional pain. However, the relief is often short-lived, leading to a cycle of guilt and further impulsive behavior
#45 No systematic or controlled psychosocial treatments.
Successful anecdotal treatments include:
Complete abstinence from prospective stores
Aversive conditioning
Systemic desensitization
Covert sensitization
Psychodynamic therapy
Antidepressants
Mood stabilizers such as Lithium
Combination therapy – Antidepressants and Mood Stabilizers
Antipsychotics
CNS – Stimulants
ECT
#47 Key Features
Recurrent Fire Setting:
Individuals with pyromania deliberately set fires on multiple occasions. This distinguishes it from other behaviors related to fire, such as accidental fire-setting or arson for profit.
Affective Arousal:
Before setting the fire, individuals often experience tension, anxiety, or affective arousal. This pre-incident emotional state is a crucial aspect of pyromania, highlighting the internal conflict that the individual faces.
Fascination with Fire:
There is a marked fascination or attraction to fire and its associated activities, including firefighting. This interest can manifest as curiosity about how fires start and the processes involved in firefighting.
Pleasure or Relief:
After setting a fire, individuals typically report feelings of pleasure, gratification, or relief. This post-incident emotional response reinforces the behavior, making it more likely to recur.
Diagnostic Criteria
For a diagnosis of pyromania, several criteria must be met:
Multiple Instances: The individual must have engaged in fire-setting on more than one occasion.
Emotional States: There should be evidence of stress or tension prior to the act and relief or gratification following it.
Not for Gain: The fire-setting behavior must not be motivated by a desire for monetary gain, revenge, or other external factors. It is a purely impulsive act.
Significant Distress: The behavior must cause significant distress or impairment in social, occupational, or other areas of functioning.
Exclusion of Other Disorders: The diagnosis should not be better explained by another mental disorder, such as conduct disorder or antisocial personality disorder.
Prevalence and Literature
Rarity: Pyromania is considered extremely rare compared to other impulse control disorders. The exact prevalence is difficult to determine due to the limited number of cases and underreporting.
Scarce Literature: There is a lack of extensive literature on pyromania, which may contribute to the challenges in understanding its etiology, treatment, and long-term outcomes
#49 Psychosocial Factors
Symbolism of Fire:
Freudian Perspective: Sigmund Freud viewed fire as a symbol of sexuality. He believed that the warmth produced by fire can evoke sensations akin to sexual arousal. Additionally, the shapes and movements of flames can be interpreted as phallic symbols, reinforcing this connection.
Behavioral Motivations:
Volunteer Firefighters: Some individuals with pyromania may be volunteer firefighters who set fires for various reasons:
Proving Bravery: They may wish to demonstrate their courage and bravery.
Forcing Action: By creating a fire, they compel other firefighters to respond, allowing them to take a leading role in the action.
Demonstrating Power: The act may be a way to showcase their ability to control and extinguish fire, reinforcing a sense of power.
Expression of Emotional Distress:
Accumulated Rage: Setting fires can be a way for individuals to vent accumulated rage stemming from feelings of social, physical, or sexual inferiority. This behavior acts as an outlet for deep-seated frustrations and emotional turmoil.
#50 Father Absence:
Impact of Absent Fathers: Studies have indicated that many individuals with pyromania come from backgrounds where their fathers were absent. This absence can lead to feelings of neglect and emotional distress.
Wish for Father’s Return: The act of fire-setting can symbolize a desire for the absent father to return, functioning as a rescuer who will extinguish the flames and alleviate the child's suffering. This dynamic underscores the emotional longing for paternal support and protection.
Biological Factors
Neurochemical Abnormalities:
Low CSF Levels: Individuals with pyromania may exhibit low levels of certain neurochemicals, particularly:
5-Hydroxyindoleacetic Acid (5-HIAA): This is a major metabolite of serotonin. Low levels in cerebrospinal fluid (CSF) indicate potential deficits in serotonergic activity, which can contribute to impulsive and aggressive behaviors.
3-Methoxy-4-hydroxyphenylglycol (MHPG): This is a metabolite of norepinephrine. Low levels suggest altered adrenergic functioning, which can further predispose individuals to impulsivity and emotional dysregulation.
Serotonergic and Adrenergic Involvement: The connection between low levels of 5-HIAA and MHPG indicates possible dysfunction in both serotonergic and adrenergic systems, which may play a role in the impulsivity characteristic of pyromania.
#53 DD
Arson
Psychosis
Impaired judgment due to substance abuse
mental retardation or dementia
Dissocial personality disorder
Mood disorders
Conduct disorders
Temporal lobe epilepsy
Learning disability
#55 N-Acetyl- Cysteine – new molecule shows promise in managing TTM, the research findings need to be communicated to mental health providers
#56 Hence to include TTM & skin picking in OC related disorder

![What is Impulsivity?
• Rapid, unplanned reactions to stimuli before complete processing of information.
• Decreased sensitivity to negative consequences of behavior.
• Lack of regard for long-term consequences.
• Impulsivity often has an impact, not only on the impulsive individual, but also on
others.
[F. Gerard Moeller, Ernest S. Barratt,2001]
• Failure to inhibit behaviors motivated by reward.
[Grant et al.2006]](https://image.slidesharecdn.com/impulsecontroldisorders-250527094704-011e845e/75/IMPULSE-CONTROL-DISORDERS-pp-for-pg-stutx-4-2048.jpg)
![What is Compulsivity?
• Failure to suppress repetitive behaviors designed to relieve
tension or reduce a negative emotion state.
[Grant et al.2006]
• Desire to avoid harm.
[Fineberg et al., 2010]](https://image.slidesharecdn.com/impulsecontroldisorders-250527094704-011e845e/75/IMPULSE-CONTROL-DISORDERS-pp-for-pg-stutx-6-2048.jpg)
![ICD-10 Habit and Impulse Disorder
• F63.0 Pathological gambling
• F63.1 Pathological fire-setting [pyromania]
• F63.2 Pathological stealing [kleptomania]
• F63.3 Trichotillomania
• F63.8 Other habit and impulse disorders
• F63.9 Habit and impulse disorder, unspecified](https://image.slidesharecdn.com/impulsecontroldisorders-250527094704-011e845e/75/IMPULSE-CONTROL-DISORDERS-pp-for-pg-stutx-12-2048.jpg)
![ICD among Parkinson's disease
• Around 3000 PD patients interviewed for ICD
• More common in patients treated with a dopamine agonist than
in patients not taking a dopamine agonist [odds ratio:2.72]](https://image.slidesharecdn.com/impulsecontroldisorders-250527094704-011e845e/75/IMPULSE-CONTROL-DISORDERS-pp-for-pg-stutx-21-2048.jpg)

![Conclusion
• Relationship between Impulsivity & compulsivity are intricate. These
symptoms overlap in many psychiatric disorders
• Limited studies on epidemiology at present. There exists tremendous
scope for research in this direction
• Evidence in neurobiology shows involvement of reward pathway including
vmPFC, OFC, Striatum[ventral to dorsum] in all ICD similar to substance use
disorder](https://image.slidesharecdn.com/impulsecontroldisorders-250527094704-011e845e/75/IMPULSE-CONTROL-DISORDERS-pp-for-pg-stutx-55-2048.jpg)