Important Obstetric Emergency that must be recognised
1.
MEDICAL OBSTETRIC EMERGENCIES
TOPICS:
Shoulderdystocia
Cord prolapse
Uterine inversion
Eclampsia
Manual removal of placenta
SUPERVISED BY:
DR YVONNE
DR REZA
PRESENTED ON:
31ST
DECEMBER 2021
2.
N A BIL A H FA R HA N A B I N T I R A M L I
SHOULDER DYSTOCIA
3.
DEFINITION
A vaginalcephalic delivery that requires additional obstetric maneuvers
to deliver the fetus after gentle downward traction has failed.
4.
PATHOPHYSIOLOGY
Anterior fetalshoulder / Posterior fetal shoulder impact on the
maternal symphysis or the sacral promontory respectively,
preventing delivery of body after delivery of fetal head,
DIAMETER OF
MATERNAL PELVIS
BISACROMIAL
DIAMETER OF
FETUS
LESS THAN
5.
RISK FACTORS
MATERNAL FETALLABOUR RELATED
Diabetes mellitus Macrosomia Long first stage of labour
Short stature Postmaturity Long second stage of labour
Previous shoulder dystocia Instrumental delivery
Obesity Induction of labour
Use of oxytocin
6.
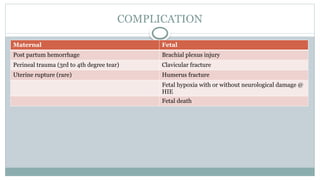
COMPLICATION
Maternal Fetal
Post partumhemorrhage Brachial plexus injury
Perineal trauma (3rd to 4th degree tear) Clavicular fracture
Uterine rupture (rare) Humerus fracture
Fetal hypoxia with or without neurological damage @
HIE
Fetal death
7.
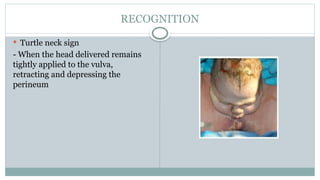
RECOGNITION
Turtle necksign
- When the head delivered remains
tightly applied to the vulva,
retracting and depressing the
perineum
8.
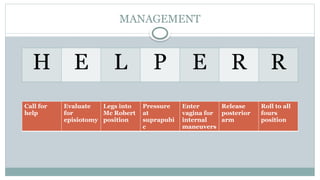
MANAGEMENT
H E LP E R R
Call for
help
Evaluate
for
episiotomy
Legs into
Mc Robert
position
Pressure
at
suprapubi
c
Enter
vagina for
internal
maneuvers
Release
posterior
arm
Roll to all
fours
position
9.
CALL FOR HELP
Senior obstetricians, midwifery staff, PAEDIATRICIAN
Inform mother to stop pushing
Do not apply fundal pressure
Bring mother to the edge of bed
10.
EVALUATE NEED FOREPISIOTOMY
Necessary only to make room if internal maneuvers is required
Shoulder dystocia is a bony impaction, so episiotomy alone will not
release the shoulder
11.
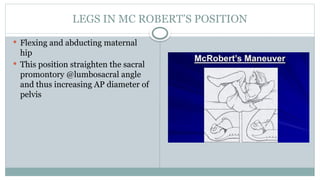
LEGS IN MCROBERT’S POSITION
Flexing and abducting maternal
hip
This position straighten the sacral
promontory @lumbosacral angle
and thus increasing AP diameter of
pelvis
12.
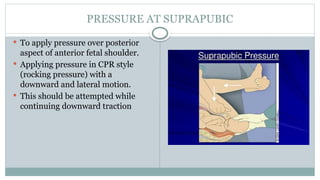
PRESSURE AT SUPRAPUBIC
To apply pressure over posterior
aspect of anterior fetal shoulder.
Applying pressure in CPR style
(rocking pressure) with a
downward and lateral motion.
This should be attempted while
continuing downward traction
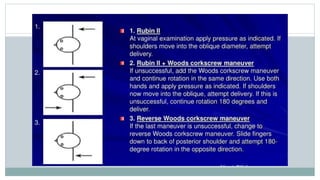
13.
ENTER PELVIS FORINTERNAL MANEUVERS
This maneuvers done to manipulate the fetus to rotate the anterior
shoulder into an oblique plane and under maternal symphysis.
15.
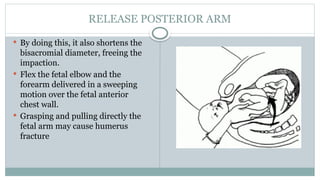
RELEASE POSTERIOR ARM
By doing this, it also shortens the
bisacromial diameter, freeing the
impaction.
Flex the fetal elbow and the
forearm delivered in a sweeping
motion over the fetal anterior
chest wall.
Grasping and pulling directly the
fetal arm may cause humerus
fracture
16.
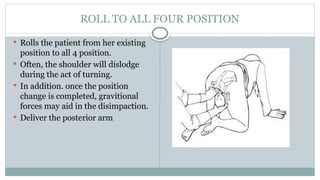
ROLL TO ALLFOUR POSITION
Rolls the patient from her existing
position to all 4 position.
Often, the shoulder will dislodge
during the act of turning.
In addition. once the position
change is completed, gravitional
forces may aid in the disimpaction.
Deliver the posterior arm
17.
IF ALL MANEUVERSFAIL...
Consider Zavanelli maneuvers, cleidotomy or symphysiotomy
Introduction
Definition: descentof the umbilical cord through the cervix
alongside or past the presenting part in the presence of ruptured
membranes
Incidence: 0.1% to 0.6
Breech : 1%
Common : male fetus
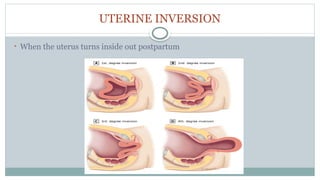
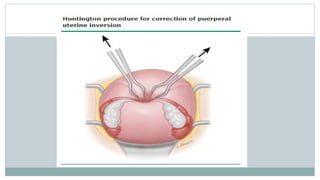
UTERINE INVERSION
Incidence-1:2000-3000 deliveries
Maternal mortality as high as 15%
Risk Factors
1. Strong traction on umbilical cord with excessive fundal pressures
2.Abnormal adherence of placenta
3.Short cord
4.Fundal implantation of placenta
5.Previous uterine inversion
29.
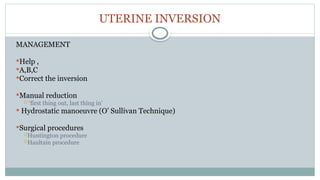
UTERINE INVERSION
CLINICAL FEATURES
1.Severeabdominal pain
2.Neurogenic shock ( disproportionate to blood loss )
3.Uterine fundus not palpable abdominally
4.Mass in vagina on VE
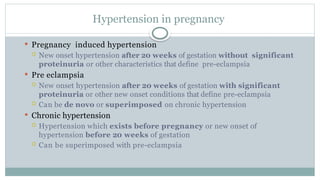
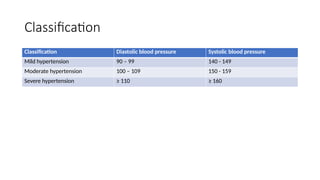
Hypertension in pregnancy
Pregnancy induced hypertension
New onset hypertension after 20 weeks of gestation without significant
proteinuria or other characteristics that define pre-eclampsia
Pre eclampsia
New onset hypertension after 20 weeks of gestation with significant
proteinuria or other new onset conditions that define pre-eclampsia
Can be de novo or superimposed on chronic hypertension
Chronic hypertension
Hypertension which exists before pregnancy or new onset of
hypertension before 20 weeks of gestation
Can be superimposed with pre-eclampsia
37.
Pre-eclampsia
New onsetof hypertension (over 140 mmHg systolic or over 90 mmHg diastolic) after 20
weeks of pregnancy and the coexistence of 1 or more of the following new-onset conditions:
proteinuria (urine protein: creatinine ratio of 30 mg/mmol or more or albumin: creatinine
ratio of 8 mg/mmol or more, or at least 1 g/litre [2+] on dipstick testing) or
other maternal organ dysfunction:
renal insufficiency (creatinine 90 micromol/litre or more, 1.02 mg/100 ml or more)
liver involvement (elevated transaminases [alanine aminotransferase or aspartate aminotransferase over 40
IU/litre] with or without right upper quadrant or epigastric abdominal pain)
neurological complications such as eclampsia, altered mental status, blindness, stroke, clonus, severe
headaches or persistent visual scotomata
haematological complications such as thrombocytopenia (platelet count below 150,000/ microlitre),
disseminated intravascular coagulation or haemolysis
uteroplacental dysfunction such as foetal growth restriction, abnormal umbilical artery
doppler waveform analysis, or stillbirth.
38.
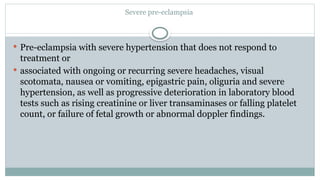
Severe pre-eclampsia
Pre-eclampsiawith severe hypertension that does not respond to
treatment or
associated with ongoing or recurring severe headaches, visual
scotomata, nausea or vomiting, epigastric pain, oliguria and severe
hypertension, as well as progressive deterioration in laboratory blood
tests such as rising creatinine or liver transaminases or falling platelet
count, or failure of fetal growth or abnormal doppler findings.
39.
Eclampsia
• Eclampsia :A convulsive condition associated with pre-eclampsia
• This may or may not be preceded by markedly elevated blood
pressure or proteinuria but usually preceded by symptoms of
impending eclampsia
• This condition can be life threatening for both the mother and fetus
40.
Eclampsia
• Some ofthe patients will present with signs & symptoms of impending eclampsia.
• However, there are no recognizable prodromal signs & symptoms in 20% of cases.
• One third of the cases occur before proteinuria and hypertension have been documented.
• It is grand mal convulsion which pass through stages of: Tonic (contraction), Clonic
(relaxation) and Coma
• Usually take about 60-90 seconds
• Whenever convulsions appears during pregnancy, delivery or the puerperium the diagnosis
of eclampsia should be made until prove otherwise
Risk factor
• Firstpregnancy ( Primigravida)
• Multiparous with –pre-eclampsia in any previous pregnancy
• Multiparous with ten years or more since last baby
• Age 40 years or more
• Body mass index of 35 or more
• Family history of pre-eclampsia (in mother or sister)
• Booking diastolic blood pressure of 80mmHg or more
• Booking proteinuria (of ≥ 1+ on more than one occasion or quantified at ≥ 0.3 g/24 hour)
• Multiple pregnancy
• Certain underlying medical conditions
• Pre-existing hypertension
• Pre-existing renal disease
• Pre-existing diabetes
• Antiphospholipid antibodies / Systemic lupus erythematous
43.
Sign and symptomsof impending eclampsia
• Severe headache
• Blurring of vision
• Epigastric pain
• Nausea and vomiting
• Clonus / brisk deep tendon reflexes
• Papilledema
• Liver tenderness
• Abnormal liver enzymes
• HELLP syndrome
• Intrauterine growth restriction
• Pulmonary edema and / or congestive cardiac failure
• Thromboembolic phenomenon
44.
Complications of Pre-eclampsia/Eclampsia
•Neurological system
•Convulsion (eclampsia)
•Cerebral oedema
•Hypertensive encephalopathy (papilledema, retinal
• haemorrhage, exudate)
• Cardiovascular system
•Greater vascular permeability
•Generalized oedema
•Heart failure
•Pulmonary oedema
•Liver
•HELLP syndrome ( haemolysis, elevation of liver enzymes, low platelets)
45.
Complications of Pre-eclampsia/Eclampsia
•Renal
•glomeruloendotheliosis
•Loss of protein
•Reduction in plasma oncotic pressure and exacerbates the development of oedema
•Hematological
•Hemolytic anemia
•Reduction in platelet count
•Disseminated intravascular coagulation
•Placenta abruptio
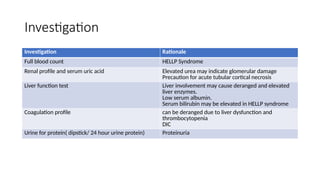
Investigation
Investigation Rationale
Full bloodcount HELLP Syndrome
Renal profile and serum uric acid Elevated urea may indicate glomerular damage
Precaution for acute tubular cortical necrosis
Liver function test Liver involvement may cause deranged and elevated
liver enzymes.
Low serum albumin.
Serum bilirubin may be elevated in HELLP syndrome
Coagulation profile can be deranged due to liver dysfunction and
thrombocytopenia
DIC
Urine for protein( dipstick/ 24 hour urine protein) Proteinuria
48.
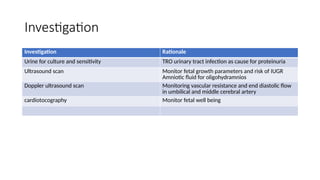
Investigation
Investigation Rationale
Urine forculture and sensitivity TRO urinary tract infection as cause for proteinuria
Ultrasound scan Monitor fetal growth parameters and risk of IUGR
Amniotic fluid for oligohydramnios
Doppler ultrasound scan Monitoring vascular resistance and end diastolic flow
in umbilical and middle cerebral artery
cardiotocography Monitor fetal well being
49.
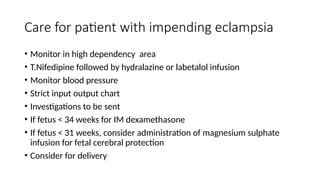
Care for patientwith impending eclampsia
• Monitor in high dependency area
• T.Nifedipine followed by hydralazine or labetalol infusion
• Monitor blood pressure
• Strict input output chart
• Investigations to be sent
• If fetus < 34 weeks for IM dexamethasone
• If fetus < 31 weeks, consider administration of magnesium sulphate
infusion for fetal cerebral protection
• Consider for delivery
50.
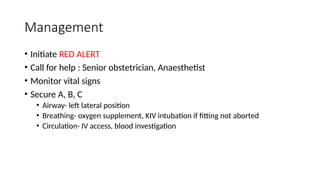
Management
• Initiate REDALERT
• Call for help : Senior obstetrician, Anaesthetist
• Monitor vital signs
• Secure A, B, C
• Airway- left lateral position
• Breathing- oxygen supplement, KIV intubation if fitting not aborted
• Circulation- IV access, blood investigation
51.
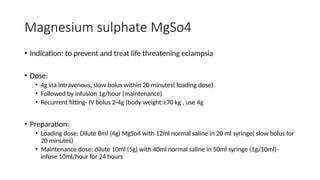
Magnesium sulphate MgSo4
•Indication: to prevent and treat life threatening eclampsia
• Dose:
• 4g via intravenous, slow bolus within 20 minutes( loading dose)
• Followed by infusion 1g/hour (maintenance)
• Recurrent fitting- IV bolus 2-4g (body weight:≥70 kg , use 4g
• Preparation:
• Loading dose: Dilute 8ml (4g) MgSo4 with 12ml normal saline in 20 ml syringe( slow bolus for
20 minutes)
• Maintenance dose: dilute 10ml (5g) with 40ml normal saline in 50ml syringe (1g/10ml)-
infuse 10ml/hour for 24 hours
52.
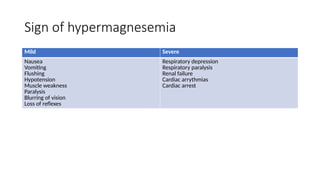
Sign of hypermagnesemia
MildSevere
Nausea
Vomiting
Flushing
Hypotension
Muscle weakness
Paralysis
Blurring of vision
Loss of reflexes
Respiratory depression
Respiratory paralysis
Renal failure
Cardiac arrythmias
Cardiac arrest
53.
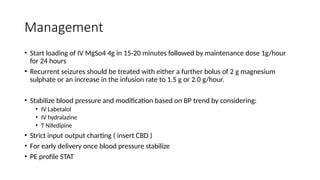
Management
• Start loadingof IV MgSo4 4g in 15-20 minutes followed by maintenance dose 1g/hour
for 24 hours
• Recurrent seizures should be treated with either a further bolus of 2 g magnesium
sulphate or an increase in the infusion rate to 1.5 g or 2.0 g/hour.
• Stabilize blood pressure and modification based on BP trend by considering:
• IV Labetalol
• IV hydralazine
• T Nifedipine
• Strict input output charting ( insert CBD )
• For early delivery once blood pressure stabilize
• PE profile STAT
54.
Management
• Fetal wellbeing
•Immediate delivery
• Second stage- instrumental delivery
• Otherwise for emergency lower segment caesarean section
• Pediatrics to standby
55.
Delivery
• Once stabilised,plans should be made to deliver
• Assessment of the fetal status by CTG/USS.
• Deliver the baby regardless of the gestational age.
56.
Precaution
• If patientis anuric, do not administer MGSO4 until urine is produced.
• Magnesium toxicity can be assessed by clinical assessment as it causes
• a loss of deep tendon reflexes (Hyporeflexia)
• respiratory depression (Desaturation)
• oliguric (<30mL/h)
• and cardiac arrest (Bradypnea)
• Altered mental status
• For those with toxicity, infusion should be halted.
• Urine output should be closely observed and if it becomes reduced below 30 ml/hour
the magnesium infusion should be halted.
• Calcium gluconate 1 g (10 ml) over 10 minutes can be given if there is concern over
respiratory depression.
57.
Post delivery observation
•To complete magnesium sulphate over 24 hours post delivery of last
seizure( whichever comes later)
• HDW or ICU admission
• Monitor magnesium sulphate toxicity
• Monitor vital signs and for blood pressure stabilization
• Watchout for complications of pre eclampsia
• Subcutaneous heparin (5000U) prophylaxis to prevent DVT
• Avoid NSAIDs for post of analgesia because of the risk of renal failure used in the presence of
severe pre-eclampsia.
• Continue MGSO4 and antihypertensive drugs.
• 25% of eclampsia will be RECURRENT in future pregnancies.
58.
Upon discharge
• Adviceon symptom of impending eclampsia
• Assessment of thromboembolism risk
• EOD BP monitoring to review back in 2 weeks at primary health
clinic
• Contraception and pap smear counselling
• Monitoring and adjustment of antihypertensive medication at
primary health clinic
Definition
• Retained placentacan be defined as
lack of expulsion of placenta within 30
minutes of delivery of the infant
• Longer the placenta remains in uterus
after delivery of baby, the greater the
risk of PPH
61.
Types
Trapped or incarceratedplacenta – separated placenta but not
delivered spontaneously or with light cord traction because the
cervix has begun to close
Placenta adherens - the placenta is adherent to
the uterine wall but easily separated manually
Placenta accreta – the placenta is pathophysically
invading the myometrium due to a defect in the decidua
62.
Risk factor
• Previousretained placenta
• Defective placental implantation
• Uterine abnormalities
• Uterine atony
• Maternal age > 30 years old
• Stillbirth
• Preterm gestational age
63.
Causes
• Placenta maybe separated but not expelled completely from uterine muscle but may still be
retained within the uterus , there are 3 causes for this retention
I. failure of the mother to push out the placenta due to exhaustion or prolonged labour
II. Closure of the cervix preventing the placenta from being expelled
III. A constriction ring in the uterus can hold up the placenta
• Simple adherent placenta – placenta may fail to separate completely from uterine muscle due to lack
of contraction the uterine muscle . This condition is called uterine atonicity which occurs due to
repeated pregnancy , prolonged labour , or overdistension of the uterus during pregnancy
64.
• Morbid adhesionof placenta – occurs when placenta is implanted deeply into uterine muscles and thus fails to
separate
• In simple cases , it is only attached firmly to muscle can be removed easily by hand . In severe morbid adhesion , the
placenta can be deeply attached through thickened muscles . There are 3 types of morbid adhesion of the placenta
I. Placenta accreta – the placenta penetrates deeply into uterine endometrium and reaches muscles but does not
penetrate into the muscle
II. Placenta increta – the placenta attaches even deeply into the uterine wall and penetrates into the muscle
III. Placenta percreta – the placenta not only penetrates through full thickness of the uterine wall but also attaches to
another organ such as bladder or rectum
65.
• RISKS
• Theremay be severe bleeding which may be life threatening
• Attempts of manual removal of placenta can cause multiple injuries to the mother such as
like vulvar hematoma , perineal tear , cervical tears and vaginal wall tears
• Management
If the placenta is undelivered within 30 minutes consider -
• Emptying bladder
• Breastfeeding or nipple stimulation
• Change of position – encourage an upright position
• If bleeding – measure blood loss , insert urinary catheter , continue oxytocin , inform
anesthetist and prepare patient for manual removal of placenta ( MROP )
66.
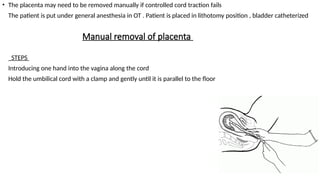
Manual removal ofplacenta
• The placenta may need to be removed manually if controlled cord traction fails
• The patient is put under general anesthesia in OT . Patient is placed in lithotomy position , bladder catheterized
• STEPS
• Introducing one hand into the vagina along the cord
• Hold the umbilical cord with a clamp and gently until it is parallel to the floor
67.
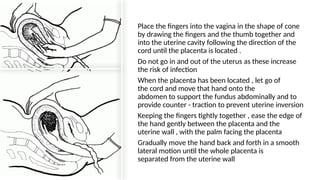
• Place thefingers into the vagina in the shape of cone
by drawing the fingers and the thumb together and
into the uterine cavity following the direction of the
cord until the placenta is located .
• Do not go in and out of the uterus as these increase
the risk of infection
• When the placenta has been located , let go of
the cord and move that hand onto the
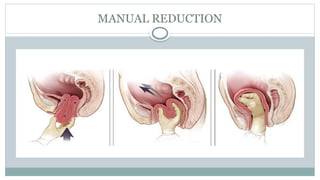
abdomen to support the fundus abdominally and to
provide counter - traction to prevent uterine inversion
• Keeping the fingers tightly together , ease the edge of
the hand gently between the placenta and the
uterine wall , with the palm facing the placenta
• Gradually move the hand back and forth in a smooth
lateral motion until the whole placenta is
separated from the uterine wall
68.
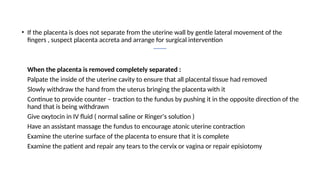
• If theplacenta is does not separate from the uterine wall by gentle lateral movement of the
fingers , suspect placenta accreta and arrange for surgical intervention
• When the placenta is removed completely separated :
Palpate the inside of the uterine cavity to ensure that all placental tissue had removed
Slowly withdraw the hand from the uterus bringing the placenta with it
Continue to provide counter – traction to the fundus by pushing it in the opposite direction of the
hand that is being withdrawn
Give oxytocin in IV fluid ( normal saline or Ringer's solution )
Have an assistant massage the fundus to encourage atonic uterine contraction
Examine the uterine surface of the placenta to ensure that it is complete
Examine the patient and repair any tears to the cervix or vagina or repair episiotomy
69.
Post procedure care
Observe
•Observe the patient closely
until the iv sedation is worn
off
Monitor
• Monitor the vital signs every
30 minutes for the next 6
hours or until stable Palpate
• Palpate the uterine fundus to
ensure that the uterus
remains contracted Check
• Check for
excessive lochia Continue
• Continue IV fluids
infusion Transfuse
• Transfuse if
necessary
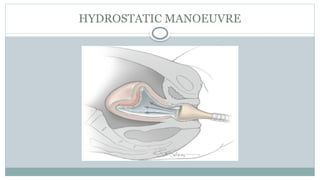
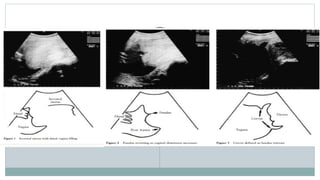
#32 After written consent for hydrostatic reduction was obtained, pethidine 100 mg was administered intramuscularly. A
20G Foley’s catheter was inserted vaginally under the subpubic angle over the attendants gloved hand. The catheter
was used for rapid infusion of 3 l of a 0.9% saline solution to hydrosufflate the vagina. An assistant provided manual
compression of the saline infusion bag. Water-tight vaginal occlusion was facilitated by straightening the patients legs to the supine position, effectively clamping the vulva about the attendant’s arm. During the procedure, lasting 9 min,
the successful reduction was recorded by sequential sonar images (Figures 1–6). Five units of oxytocin and 1 g of cephazolin were then given intravenously. The patients hematocrit had dropped to 21% and 3 units of fresh packed cells were transfused
https://obgyn.onlinelibrary.wiley.com/doi/pdf/10.1046/j.1469-0705.1998.12040283.x
#34 In the Huntington procedure, the cup formed by the inversion is located. A clamp, such as an Allis or Babcock clamp, is placed on each round ligament entering the cup, approximately 2 cm deep in the cup. Gently pulling on the clamps exerts upward traction on the inverted fundus. Clamping and traction are repeated until the inversion is corrected. The myometrium can be clamped if the round ligaments cannot be identified.

![Pre-eclampsia
New onset of hypertension (over 140 mmHg systolic or over 90 mmHg diastolic) after 20
weeks of pregnancy and the coexistence of 1 or more of the following new-onset conditions:
proteinuria (urine protein: creatinine ratio of 30 mg/mmol or more or albumin: creatinine
ratio of 8 mg/mmol or more, or at least 1 g/litre [2+] on dipstick testing) or
other maternal organ dysfunction:
renal insufficiency (creatinine 90 micromol/litre or more, 1.02 mg/100 ml or more)
liver involvement (elevated transaminases [alanine aminotransferase or aspartate aminotransferase over 40
IU/litre] with or without right upper quadrant or epigastric abdominal pain)
neurological complications such as eclampsia, altered mental status, blindness, stroke, clonus, severe
headaches or persistent visual scotomata
haematological complications such as thrombocytopenia (platelet count below 150,000/ microlitre),
disseminated intravascular coagulation or haemolysis
uteroplacental dysfunction such as foetal growth restriction, abnormal umbilical artery
doppler waveform analysis, or stillbirth.](https://image.slidesharecdn.com/obstetricemergency-250809160342-c23b07d6/85/Important-Obstetric-Emergency-that-must-be-recognised-37-320.jpg)




























![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















