Download to read offline

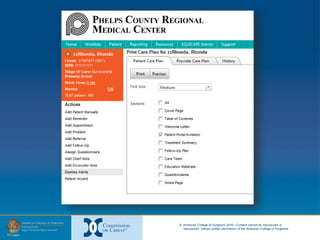
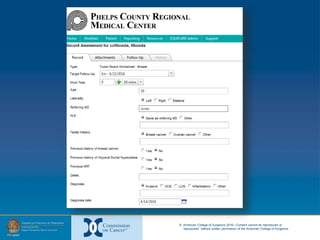
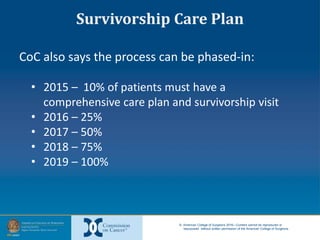
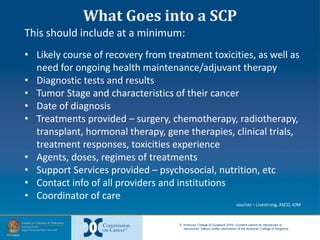
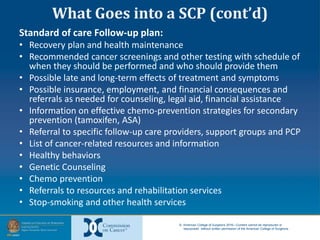

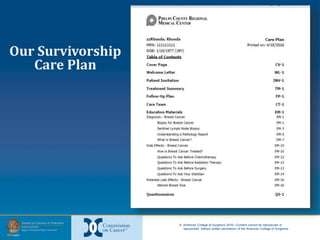

The document provides information on developing and implementing survivorship care programs that meet Commission on Cancer (CoC) accreditation standards. It discusses how PCRMC in Rolla, Missouri established their survivorship care processes over time to meet these standards, including developing a navigation process, integrating distress screening, and creating survivorship care plans. The document offers advice on using regulations, existing staff, and starting the process at the beginning of a patient's cancer journey to establish survivorship programs efficiently.








































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















