
Recommended
More Related Content
What's hot
Similar to Impetigo
Similar to Impetigo (20)
More from vikasaagrahari007
More from vikasaagrahari007 (12)
Recently uploaded
Recently uploaded (20)
Impetigo
- 2. IMPETIGO • Impetigo is a superficial skin infection that is seen most commonly in children. • The infection is generally classified as bullous or non-bullous based on clinical presentation. • Impetigo is most common during hot, humid weather, which facilitates microbial colonization of the skin • Minor trauma, such as scratches or insect bites, allows entry of organisms into the superficial layers of skin, and infection ensues. • Impetigo is highly communicable and readily spreads through close contact, especially among siblings and children in
- 3. ETIOLOGY Most cases of impetigo were caused by Streptococcus pyogenes, but recently Staphylococcus aureus, either alone or in combination with S. pyogenes, has emerged as the principal cause of impetigo.
- 4. Epidemiology: • The bullous form most frequently affects neonates and accounts for approximately 10% of all cases of impetigo • Based on data from studies published since 2000 from low and low-middle income countries, we estimate the global population of children suffering from impetigo at any one time to be in excess of 162 million, predominantly in tropical, resource-poor contexts. Impetigo is an under-recognised disease and in conjunction with scabies, comprises a major childhood dermatological condition with potential lifelong consequences if untreated.
- 5. Occurrence • On exposed skin mainly on face. • Most common during hot, humid weather, which facilitates microbial colonization of the skin. • Minor trauma, such as scratches or insect bites, then allows entry of organisms into the superficial layers of skin, and infection ensues.
- 7. STAGES OF IMPETIGO BY TYPE • There are three types of impetigo based on the bacteria that cause them and the sores they form. Each type goes through a series of stages. 1. Non Bullous impetigo 2. Bullous impetigo 3. Ecthyma
- 8. NON -BULLOUS • Non-bullous impetigo is mainly caused by Staphylococcus aureus. It’s the most common form of impetigo. • It goes through the following stages: • It usually starts with reddish, itchy sores around the mouth and nose. • The sores break open, leaving red and irritated skin around them. • A brownish-yellow crust
- 9. BULLOUS IMPETIGO • Bullous impetigo is almost always caused by Staphylococcus aureus bacteria. • It usually forms larger blisters or bullae filled with a clear fluid that may become darker and cloudy. The blisters start on unbroken skin and aren’t surrounded by reddish areas. • The blisters become limp and clear, and then burst open. • A yellowish, crusty sore forms over the area where the blisters broke open
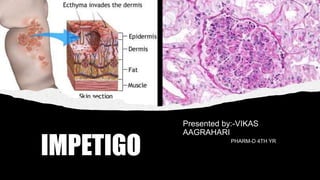
- 10. ECTHYMA • This more serious infection is much less common. It occasionally happens when impetigo isn’t treated. Ecthyma goes deeper into the skin than the other forms of impetigo, and it’s more severe. • The infection forms painful blisters on the skin of the buttocks, thighs, legs, ankles, and feet. • The blisters turn into pus- filled sores with a thicker crust. • Often, the skin around the sores turns red.
- 11. CLINICAL MANIFESTATION General • Exposed skin, especially the face, is the most common site for impetigo. Symptoms • Pruritus is common, and scratching of the lesions may further spread infection through excoriation of the skin. • Other systemic signs of infection are minimal. • Weakness, fever, and diarrhea sometimes are seen with bullous impetigo.
- 12. Signs • Non-bullous impetigo manifests initially as small, fluid- filled vesicles. • These lesions rapidly develop into pus-filled blisters that rupture readily. • Purulent discharge from the lesions dries to form golden yellow crusts that are characteristic of impetigo. • In the bullous form of impetigo, the lesions begin as vesicles and turn into bullae containing clear yellow fluid. • Bullae soon rupture, forming thin, light brown crusts.
- 13. PATHOPHYSIOLOGY-IMPETIGO • Bullous impetigo is caused by staphylococci producing exfoliative toxin that contains serine proteases acting on desmoglein, a structurally critical peptide bond in a molecule that holds epidermal cells together. This process allows Staphylococcus aureus to spread under the stratum corneum in the space formed by the toxin, causing the epidermis to split just below the stratum granulosum. Large blisters then form in the epidermis with neutrophil . In bullous impetigo, the bullae rupture quickly, causing superficial erosion and a yellow crust. •while in non-bullous impetigo, Streptococcus typically produces a thick-walled pustule with an erythematous base. Histology of non- bullous established lesions shows a thick surface crust composed of serum and neutrophils in various stages of breakdown with
- 14. Non-bullous impetigo Non bullous impetigo starts as a pink macule that evolves into a vesicle or pustule and then into crusted erosions. Untreated impetigo usually resolves within 2 to 4 weeks without scarring.
- 15. DIAGNOSIS •Cultures should be collected. •Crusted tops of lesions should be raised so that purulent material at the base of the lesion can be cultured. •Cultures should not be collected from open, draining skin pustules because they may be colonized with staphylococci and other normal skin flora. Laboratory Tests Other Diagnostic Tests :-A complete blood count is often performed
- 16. TREATMENT ORAL ADULT DOSE • Dicloxacillin 250–500 mg every 6 h • Cephalexin 250–500 mg every 6 h • Cefadroxil 500 mg every 12 h • Clindamycin 150–300 mg every 6–8 • Mupirocin ointment every 8 ha ORAL PEDIATRIC DOSE • Dicloxacillin 25–50 mg/kg in four divided doses • Cephalexin 25–50 mg/kg in two to four divided doses • Cefadroxil 30 mg/kg in two divided doses • Clindamycin 10–30 mg/kg/day in three to four divided doses • Mupirocin ointment every 8 ha
- 18. MONITORING PARAMETERS • Clinical response should be seen within 7 days of initiating antimicrobial therapy for impetigo. Treatment failures could be a result of noncompliance or antimicrobial resistance. • A follow-up culture of exudates should be collected for culture and sensitivity, with treatment modified accordingly • Fingernails should be kept short, and patients should be advised not to scratch any lesions to avoid spread of infection.
- 19. EDUCATION • Patients should be instructed on use of antibacterial soaps. • Avoidance of sharing of towels and washcloths, because impetigo is extremely contagious. • Children attending day care should be removed until 48 to 72 hr after initiation of antibiotic treatment.
- 20. References • Craft, N, Lee PK, et al. “Superficial cutaneous infections and pyodermas.” In: Wolff K, Goldsmith LA, et al. Fitzpatrick’s Dermatology in General Medicine (seventh edition). McGraw Hill Medical, New York, 2008: 1695-8. • Habif TP, Campbell, JL, et al. “Impetigo.” In: Dermatology DDxDeck. Mosby Elsevier, China, 2006: Card#46. • Halpern AV and Heymann WR. “Bacterial diseases.” In: Bolognia JL, et al. Dermatology. (second edition). Mosby Elsevier, Spain, 2008:1075-6.