INTRODUCTION
• The 2024Guidelines define hypertension as a confirmed
office systolic BP of ≥140 mmHg or diastolic BP of ≥90 mmHg.
• confirmation is recommended with out-of-office
measurements (HBPM or ABPM) or at least one repeat office
measurement at a subsequent visit.
• Second, most adults with BP above this threshold are at
increased CVD risk, typically with 10-year risk estimates of
≥10% for fatal and non-fatal CVD events.
3.
•Current global guidelinesrecommend treating
hypertension based on
•24-h ambulatory blood pressure monitoring (ABPM)
• and home blood pressure (BP) measurements rather
than measurement in the clinical setting.
4.
• Hypertension isdefined as office SBP values >_140 mmHg and/or
diastolic BP (DBP) values >_90 mmHg.
• This is based on evidence from multiple RCTs that treatment of
patients with these BP values is beneficial.
• The same classification is used in younger, middle-aged, and older
people, whereas BP centiles are used in children and teenagers
5.
Prevalence of hypertension
•the global prevalence of hypertension was estimated to be 1.13
billion in 2015, with a prevalence of over 150 million in central and
eastern Europe.
• The overall prevalence of hypertension in adults is around 30 - 45%,
with a global age standardized prevalence of 24 and 20% in men and
women, respectively, in 2015.
• This high prevalence of hypertension is consistent across the world,
irrespective of income status, i.e. in lower, middle, and higher income
countries.
6.
•Hypertension is morecommon with advancing age,
with a prevalence of >60% in people aged >60 years.
•It is estimated that the number of people with
hypertension will increase by 15–20% by 2025,
reaching close to 1.5 billion
7.
Demographic characteristics andlaboratory
parameters
• Sex (men >women)
• Age
• Smoking (current or past history)a
• Total cholesterol and HDL-C
• Uric acid
• Diabetes
• Overweight or obesity
• Family history of premature CVD (men aged
EPIDEMIOLOGY
• Worldwide prevalenceis around 20% , and approximately 7.1 million deaths
per year may be attributable to hypertension
• The WHO reports that suboptimal BP (>115 mmHg SBP) is responsible for
62 percent of cerebrovascular disease and 49 percent of ischemic heart
disease (IHD)
• Suboptimal BP is top attributable risk factor for death throughout the world
Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United
States, 1988- 2000. JAMA 2003;290:199-206
10.
Global Burden ofHypertension:
Analysis of Worldwide Data
Kearney PM et al. Lancet 2005; 365:217-223
• In 2000, 26.4% (95% CI 26.0-26.8%) of the
adult population had hypertension, 26.6% of
men & 26.1% of women.
• By 2025, 29.2% (28.8-9.7%) were projected to
be hypertensive, 29.0% of men & 29.5% of
women.
11.
HYPERTENSION PREVALANCE- AFRICA
•Increasing prevalence rates
• Prevalence in Nigeria is reported to be 12%-22% in people
above 15 years
Kenya (1929) – no hypertension in 1800 admissions
Ghana (urban) – increase from 8% (1990) to 28% (2004)
Tanzania (1997) -26% (rural), 37% (urban)
S.Africa up to 50-60% above 65years
12.
Attributable Risk
• Onlyhalf of the burden seen in people with hypertension
(BP > 140 mmHg); remainder in prehypertensives (BP > 115mmHg)
• > 80% of the burden seen in low-income and middle-income
regions
• Over half occurred in people aged 45-69 yrs
54% stroke
47% IHD
25% other CVD
13.5% Total mortality
Study by Int Society of hypertension; Lancet May 2008;371:1513-8
13.
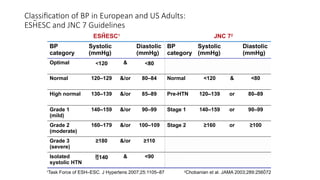
Classification of BPin European and US Adults:
ESHESC and JNC 7 Guidelines
BP
category
Systolic
(mmHg)
Diastolic
(mmHg)
BP
category
Systolic
(mmHg)
Diastolic
(mmHg)
Optimal <120 & <80
Normal 120–129 &/or 80–84 Normal <120 & <80
High normal 130–139 &/or 85–89 Pre-HTN 120–139 or 80–89
Grade 1
(mild)
140–159 &/or 90–99 Stage 1 140–159 or 90–99
Grade 2
(moderate)
160–179 &/or 100–109 Stage 2 ≥160 or ≥100
Grade 3
(severe)
≥180 &/or ≥110
Isolated
systolic HTN
140 & <90
JNC 72
ESHESC1
1
Task Force of ESH–ESC. J Hypertens 2007;25:1105–87 2
Chobanian et al. JAMA 2003;289:256072
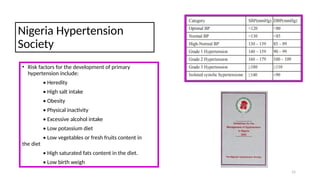
Nigeria Hypertension
Society
• Riskfactors for the development of primary
hypertension include:
• Heredity
• High salt intake
• Obesity
• Physical inactivity
• Excessive alcohol intake
• Low potassium diet
• Low vegetables or fresh fruits content in
the diet
• High saturated fats content in the diet.
• Low birth weigh
15
17.
• In 2000,972 million adults had hypertension; 333 million
(329-336 million) in economically developed countries & 639
million (625-654 million) in economically developing
countries.
• By 2025, the number of adults with hypertension was
predicted to increase by about 60% to a total of 1.56 billion.
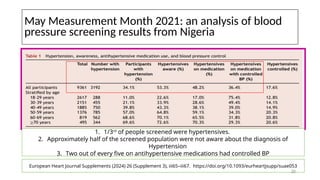
May Measurement Month2021: an analysis of blood
pressure screening results from Nigeria
European Heart Journal Supplements (2024) 26 (Supplement 3), iii65–iii67. https://doi.org/10.1093/eurheartjsupp/suae053
1. 1/3rd
of people screened were hypertensives.
2. Approximately half of the screened population were not aware about the diagnosis of
Hypertension
3. Two out of every five on antihypertensive medications had controlled BP
20
21.
Causes
• The majority(80–90%) of patients with hypertension have primary
elevation of blood pressure, i.e. essential hypertension of unknown
cause.
• Essential hypertension has a multifactorial aetiology.
22.
Genetic factors
• Bloodpressure tends to run in families and children of hypertensive
parents tend to have higher blood pressure than age-matched
children of parents with normal blood pressure.
• This familial concordance of blood pressure may be explained, at least
in part, by shared environmental influences.
23.
Fetal factors
• Lowbirth weight is associated with subsequent high blood
pressure. This relationship may be due to fetal adaptation to
intrauterine undernutrition with long-term changes in blood vessel
structure or in the function of crucial hormonal systems.
24.
Environmental factors
• Amongstthe several environmental factors the following are
significant:
• Obesity.
• Fat people have higher blood pressures than thin people. There is a
risk of overestimation if the blood pressure is measured with a
small cuff.
• Sleep disordered breathing often seen with obesity may be an
additional risk factor.
25.
• Alcohol intake.
•Most studies have shown a close relationship between the
consumption of alcohol and blood pressure level.
• However, subjects who consume small amounts of alcohol seem to
have lower blood pressure level than those who consume no
alcohol.
26.
Sodium intake.
• Ahigh sodium intake has been suggested to be a major determinant
of blood pressure differences between and within populations around
the world.
• Populations with higher sodium intakes have higher average blood
pressures than those with lower sodium intake.
• Migration from a rural to an urban environment is associated with an
increase in blood pressure that is in part related to the amount of salt
in the diet.
27.
• Stress.
• Whilstacute pain or stress can raise blood pressure, the relationship
between chronic stress and blood pressure is uncertain.
28.
Humoral mechanisms
• Theautonomic nervous system,
• the renin– angiotensin,
• natriuretic peptide and
• kallikrein–kinin system, plays a role in the physiological regulation of
short-term changes in blood pressure and have been implicated in
the pathogenesis of essential hypertension.
• A low renin, salt sensitive, essential hypertension in which patients
have renal sodium and water retention has been described.
29.
Insulin resistance
• Anassociation between diabetes and hypertension is recognized and
a syndrome has been described of hyperinsulinaemia, glucose
intolerance, reduced levels of HDL cholesterol, hypertriglyceridaemia
and central obesity (all of which are related to insulin resistance) in
association with hypertension.
• This association (also called the ‘metabolic syndrome is a major risk
factor for cardiovascular disease.
30.
Secondary hypertension
• Secondaryhypertension is where blood pressure elevation is the result of a
specific and potentially treatable cause.
• Secondary forms of hypertension include the following:
• Renal diseases
• These account for over 80% of the cases. The common causes are:
diabetic nephropathy
chronic glomerulonephritis
adult polycystic disease ■
Chronic tubulointerstitial nephritis ■
renovascular disease.
31.
• Hypertension canitself cause or worsen renal disease.
• The mechanism of this blood pressure elevation is due to sodium and
water retention, although there can be inappropriate elevation of
plasma renin levels.
32.
Endocrine causes
• Theseinclude:
Conn’s syndrome
adrenal hyperplasia
phaeochromocytoma
Cushing’s syndrome
acromegaly.
Congenital cardiovascular causes is coarctation of the aorta.
33.
Drugs
• Many drugsmay cause or aggravate hypertension, or interfere with
the response to some antihypertensive agents:
• NSAIDs, oral contraceptives, steroids carbenoxolone, liquorice,
sympathomimetics and vasopressin.
• Patients taking monoamine oxidase inhibitors who consume
tyramine-containing foods may develop paroxysms of severe
hypertension.
34.
Pathophysiology
• The pathogenesisof essential hypertension is unclear.
• In some young hypertensive patients, there is an early increase in
cardiac output, in association with increased pulse rateand
circulating catecholamines.
• This could result in changes in baroreceptor sensitivity, which would
then operate at a higher blood pressure level.
• In chronic hypertension , the cardiac output is normal and it is an
increased peripheral resistance that maintains the elevated blood
pressure.
35.
• The resistancevessels (the small arteries and arterioles) show
structural changes in hypertension with an increase in wall thickness
and a reduction in the vessellumen diameter.
• There is also some evidence for rarefaction (decreased density) of
these vessels.
• These mechanisms would result in an increased overall peripheral
vascular resistance.
36.
• Hypertension alsocauses changes in the large arteries.
• There is thickening of the media, an increase in collagen and the
secondary deposition of calcium.
• These changes result in a loss of arterial compliance, which in turn
leads to a more pronounced arterial pressure wave.
• Pulse wave velocity is a measure of arterial stiffness and is inversely
related to distensibility. With each systolic contraction a pulse wave
travels down the arterial wall before the flow of blood.
37.
• Thus, themore rigid the arterial wall, the faster the wave travels. It
can be measured but is not in routine use.
• Atheroma develops in the large arteries owing to the interaction of
these mechanical stresses and low growth factors.
• Endothelial dysfunction with alternations in agents such as nitric
oxide and endothelins appear to be involved
38.
• Changes inthe renal vasculature eventually lead to a reducedrenal
perfusion, reduced glomerular filtration rate and, finally, a reduction
in sodium and water excretion.
• The decreased renal perfusion may lead to activation of the renin–
angiotensin system (renin converts angiotensinogen to angiotensin I,
which is in turn converted to angiotensin II by angiotensin-converting
enzyme) with increased secretion of aldosterone and further
sodium and water retention.
39.
Complications
• Cerebrovascular disease
•coronary artery disease
• renal failure and
• peripheral vascular disease.
• Hypertensives have a sixfold increase in stroke (both haemorrhagic
and atherothrombotic).
• There is a threefold increase in cardiac death (due either to coronary
events or to cardiac failure). Furthermore, peripheral arterial
disease is twice as common.
40.
EVIDENCE OF TARGETORGAN DAMAGE
AND CARDIOVASCULAR DISEASE
• Cardiac LVH (moderate to severe)
Systolic or diastolic dysfunction
Ischemic heart disease
• Vasculature Peripheral arterial disease
Carotid arterial disease
Aortic aneurysm
• Renal Albuminuria (urinary albumin >300 mg/day)
CKD (estimated GFR <60 mL/min) or
• Cerebrovascular Stroke /Transient ischemic attack
Malignant hypertension
• Malignantor accelerated hypertension occurs when blood pressure
rises rapidly and is considered with severe hypertension (diastolic
blood pressure > 120 mmHg).
• The characteristic histological change is fibrinoid necrosis of the
vessel wall and, unless treated, it may lead to death from progressive
renal failure, heart failure, aortic dissection or stroke.
• The changes in the renal circulation result in rapidly progressive renal
failure, proteinuria and haematuria.
43.
• There isalso a high risk of cerebral oedema and haemorrhage with
resultant hypertensive encephalopathy.
• In the retina there may be flame-shaped haemorrhages, cotton wool
spots, hard exudates and papilloedema.
• Without effective treatment there is a 1-year survival of less than
20%.
44.
Assessment
• Management shouldbe considered in three stages:
• assessment,
• non-pharmacological treatment and
• drug treatment.
During the assessment period, secondary causes of hypertension
should be excluded, target-organ damage from the blood pressure
should be evaluated and any concomitant conditions (e.g.
dyslipidaemia or diabetes) that may add to the cardiovascular
burden should be identified.
45.
History
• The patientwith mild hypertension is usually asymptomatic.
• Attacks of sweating, headaches and palpitations point towards the
diagnosis of phaeochromocytoma.
• Higher levels of blood pressure may be associated with headaches,
epistaxis or nocturia.
• Breathlessness may be present owing to left ventricular hypertrophy
or cardiac failure,
• angina or symptoms of peripheral arterial vascular disease suggest
the diagnosis of atheromatous renal artery stenosis.
46.
• Fibromuscular diseaseof the renal arteries encompasses a group
of conditions in which fibrous or muscular proliferation results in
morphologically simple or complex stenosis and tends to occur in
younger patients.
• Malignant hypertension may present with severe headaches, visual
disturbances, fits, transient loss of consciousness or symptoms of
heart failure.
47.
Examination
• Elevated bloodpressure is usually the only abnormal sign.
• Signs of an underlying cause should be sought, such as renal artery bruits in
renovascular hypertension, or radiofemoral delay in coarctation of the aorta.
• The cardiac examination may also reveal features of left ventricular
hypertrophy and a loudaortic second sound.
• If cardiac failure develops, there may be a sinus tachycardia and a
third heart sound.
• Fundoscopy is an essential part of the examination of any hypertensive
patient. The abnormalities are graded according to the Keith–Wagener
classification:
48.
• Grade 1–tortuosity of the retinal arteries with increased
reflectiveness (silverwiring).
• Grade 2 – grade 1 plus the appearance of arteriovenous nipping
produced when thickened retinal arteries pass over the retinal
veins.
• Grade 3 – grade 2 plus flame-shaped haemorrhages and soft
(‘cotton wool’) exudates actually due to small infarcts
• Grade 4 – grade 3 plus papilloedema (blurring of the margins
of the optic disc).
• Grades 3 and 4 are diagnostic of malignant hypertension.
49.
Ambulatory blood pressuremonitoring
• Indirect automatic blood pressure measurements can be made over
a 24-hour period using a measuring device worn by the patient.
• The clinical role of such devices remains they are used to confirm the
diagnosis in those patients with ‘white-coat’ hypertension, i.e. blood
pressure is completely normal at all stages except during a clinical
consultation.
• These patients do not have any evidence of target-organ damage, and
unnecessary treatment can be avoided.
50.
• These devicesmay also be used to monitor the response of patients
to drug treatment and to determine the adequacy of 24hour control
with once-daily medication.
• Ambulatory blood pressure recordings is a better predictor of
cardiovascular risk than clinic measurements.
• Analysis of the diurnal variation in blood pressure suggests that
those hypertensives with loss of the usual nocturnal fall in blood
pressure (‘non-dippers’) have a worseprognosis than those who
retain this pattern.
51.
Investigations
• Routine investigationinclude:
• ECG
• urine stix test for protein and blood
• fasting blood for lipids (total and HDL cholesterol) and glucose
• Serum urea, creatinine and electrolytes
52.
• If theurea or creatinine is elevated, more specific renal investigations
are indicated – creatinine clearance, renal ultrasound (in case of polycystic
kidney disease, or parenchymal renal artery disease) and a renal isotope scan
or renal angiography if renovascular disease (either atheromatous or
fibromuscular dysplasia) is suspected.
• A low serum potassium may indicate an endocrine disorder (either primary
hyperaldosteronism or glucocorticoid excess), and aldosterone, cortisol and
renin measurements must then be made, preferably prior to initiating
pharmacological therapy.
• Clinical suspicion of phaeochromocytoma should be investigated further with
measurement of urinary metanephrines and plasma or urinary catecholamines.
53.
• If theECG shows evidence of coronary artery disease the coronary
vascular status should be assessed.
• If left ventricular hypertrophyis suspected echocardiography (or
MRI) should be undertaken.
• A chest X-ray is indicated if cardiac involvement or aortic coarctation
is likely.
Treatment
• There shouldbe a period of assessment with repeated blood pressure
measurements, combined with advice and non Pharmacological
measures prior to theinitiation of drug therapy.
• Use of non-pharmacological therapy in include
■ weight reduction – BMI should be < 25 kg/m2
■ low-fat and saturated fat diet
■ low-sodium diet – < 6g sodium chloride per day
■
56.
• Limited alcoholconsumption – ≤ 21units/week for men and ≤ 14
units/week for women
• Dynamic exercise – at least 30 minutes’ brisk walk perday
• increased fruit and vegetable consumption
• reduce cardiovascular risk by stopping smoking and
increasing oily fish consumption.
57.
Pharmacological therapy
• Theinitiation of antihypertensive therapy in subjects with
sustained systolic blood pressure (BP) ≥ 160 mmHg, or sustained
diastolic BP ≥ 100 mmHg.
• Decide on treatment in subjects with sustained systolicblood
pressure between 140 and 159 mmHg, or sustained diastolic BP
between 90 and 99 mmHg, according to the presence or absence
of target organ damage or a 10-year cardiovascular disease risk >
20%.
• ■
58.
• In patientswith diabetes mellitus, the initiation of
antihypertensive drug therapy if systolic BP is sustained ≥ 140
mmHg, or diastolic BP is sustained ≥ 90 mmHg. ■
59.
Target blood pressure
•For most patients a target of ≈ 140 mmHg systolic blood pressure
and ≈ 85 mmHg diastolic blood pressure is recommended.
• For patients with diabetes, renal impairment or established
cardiovascular disease a lower target of ≈ 130/80 mmHg is
recommended.
• When using ambulatory blood pressure readings, mean daytime
pressures are preferred and this value would be expected to be
approximately 10/5 mmHg lower than the clinic blood pressure
equivalent for both thresholds and targets.
60.
What are thegoals of therapy?
•<140/90 for patients without diabetes or renal disease
•Most patients who achieve their systolic goal will
also achieve their diastolic goal
•<130/80 for patients with diabetes or renal disease
JNC 7
61.
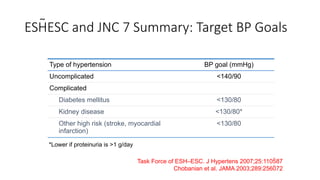
ESHESC and JNC7 Summary: Target BP Goals
Type of hypertension BP goal (mmHg)
Uncomplicated <140/90
Complicated
Diabetes mellitus <130/80
Kidney disease <130/80*
Other high risk (stroke, myocardial
infarction)
<130/80
Task Force of ESH–ESC. J Hypertens 2007;25:110587
Chobanian et al. JAMA 2003;289:256072
*Lower if proteinuria is >1 g/day
62.
• All ofthe drugs used to treat hypertension have side-effects and,
since the benefits of drug treatment are not immediate, compliance
may be a major problem. Several classes of drugs are available to
treat hypertension. The usual are:
• (a) ACE inhibitors or angiotensin receptor antagonists;
• (b) beta-blockers;
• (c) calcium-channel blockers; or
• (d) diuretics.
63.
Drug classes
• DIURETICS:Thiazide e.g
bendrofluathizide 1.25- 5 mg
• CENTRALLY ACTIING DRUGS:
Reserpine in BRINERDIN .
• ALPHA RECEPTORS BLOCKERS eg
prasosin in MINIPRES
• BETA-RECEPTOR BLOCKERS:
Atenolol in TERNOMIN
• CALCIUM ANTAGONISTS: e.g
Nifedipine in ADALAT
• ACE INHIBITORS: e.g Lisinipril in
ZESTRIL ACE RECEPTOR BLOCKERS:
e.g Telmisartan in DIOVAN
• CENTRALLY ACTING SYMPATETIC
AMINES: Methyldopa 250-2000mg
daily in 1-4 divided doses. (Avoid large
doses because of adverse reaction on
the liver.
• VASODILATORS: Hydralazine 25-200 mg
in up to 4 divided doses-useful in
resistant hypertension.
• Newer drugs
Vasopeptidase inhibitors
Oral anti renin drugs
Endothelin inhibitors
64.
Diuretics
• Thiazide diureticssuch as bendroflumethiazide (2.5–5mg daily) and
cyclopenthiazide (0.25–0.5 mg daily) are well established agents which
have been shown to reduce the risk of stroke in patients with
hypertension.
• The lower doses seems to be equally effective as higher doses in the
reduction of blood pressure and most have a duration of up to 24
hours. The major concern with these agents is their adverse metabolic
effects, particularly increased serum cholesterol, impaired glucose
tolerance, hyperuricaemia (which may precipitate gout) and
hypokalaemia. These tend to occur with higher doses of thiazide
diuretics.
65.
• Loop diureticssuch as furosemide (40 mgdaily)do have a
hypotensive effect, but are not routinely used in the treatment of
essential hypertension.
• Potassium-sparing diuretics such as amiloride (5–10 mg daily)or
spironolactone (50– 200 mg daily) are not effective agents when used
alone, with the exception of spironolactone in the treatment of
hypertension and hypokalaemia associated with primary
hyperaldosteronism.
66.
Beta-adrenoceptor blockers
• Beta-blockersare no longer a preferred initial therapy for
hypertension.
• beta-blockers are used in younger people, particularly those with an
intolerance or contraindication to ACE inhibitors and angiotensin-II
receptor antagonists; women of child-bearing potential; or
patients with evidence of increased sympathetic drive.
• In these circumstances, if therapy is initiated with a beta-blocker and
a second drug is required, add a calcium-channel blocker Rather than
a thiazide-type diuretic to reduce the patient’s risk of developing
diabetes.
67.
• Beta-blockers exerttheir effects by attenuating the effects of the
sympathetic nervous andthe renin–angiotensin systems. The major side-
effects of this classof agents are bradycardia, bronchospasm, cold
extremities, fatigue, bad dreams and hallucinations.
• These agents are especially useful in the treatment of patients with both
hypertension and angina. The drugs include atenolol (50 mg daily),
bisoprolol (10–20mg daily), metoprolol (100– 200mg in divided doses
daily) and propranolol (160–320 mg in divided doses daily).
• Atenolol has been shown to reduce brachial arterial pressure
but not aortic pressure, which is more significant in causing strokes
and heart attacks.
68.
Angiotensin-converting enzyme (ACE)
inhibitors
•These drugs block the conversion of angiotensin I to angiotensin
II, which is a potent vasoconstrictor.
• They also block the degradation of bradykinin, a potent vasodilator.
There is evidence that black African patients respond less well to
ACE inhibitors unless combined with diuretics.
• They are useful in diabetics with nephropathy, where they have been
shown to slow disease progression, and in those patients with
symptomatic or asymptomatic left ventricular dysfunction, where
they have been shown to improve survival.
69.
• The majorpotential side-effects are profound hypotension following
the first dose, which is usually seen in sodium depleted patients or
in those on treatment with large doses of diuretics, and deterioration
of renal function inthose with severe bilateral renovascular disease
(in whom the production of angiotensin II is playing a major role
in maintaining renal perfusion by causing efferent arteriolar
constriction at the glomerulus).
• They also cause mild dry cough in a number of patients, especially
if prescribed at high doses, due to their effect on bradykinin. These
are several ACE
70.
• These areseveral ACE inhibitors available.
• The drugs include enalapril (10–20mg daily),
• captopril (50–150mg daily)
• Ramipril (2.5– 10 mg daily),
• lisinopril (10–20 mg daily) and
• trandolapril (1– 4 mg daily).
71.
Angiotensin II receptorantagonists
• This group of agents selectively block the receptors for angiotensin
II. They share many of the actions of ACE inhibitors but, since
they do not have any effect on bradykinin, do not cause a cough.
They are currently used for patients who cannot tolerate ACE
inhibitors because of persistent cough.
• Angioneurotic oedema and renal dysfunction are encountered less
with these drugs than with ACE inhibitors. The agents include
losartan (50–100 mg daily), candesartan (up to 32 mg daily), valsartan
(80–160mg daily), irbesartan (75– 300 mg daily) and telmisartan (20–
80 mg/daily).
72.
Calcium-channel blockers
• Theseagents effectively reduce blood pressure by causing arteriolar
dilatation, and some also reduce the force of cardiac contraction. Like
the beta-blockers, they are especially useful in patients with
concomitant ischaemic heart disease. The major side-effects are
particularly seen with the
73.
• short-acting agentsand include headache, sweating, swelling of the
ankles, palpitations and flushing.
• Many of these side-effects can be lessened by the co-administration
of a beta- locker.
• The short-acting agents, such as nifedipine (10–20 mg three times
daily) are being replaced by once daily agents that are very well
tolerated and include amlodipine (5–10 mg daily), felodipine (5–20
mg daily) and long-acting nifedipine (20–90 mg daily).
74.
Alpha-blockers
• These agentscause post synaptic α1-receptor blockade with
resulting vasodilatation and blood pressure reduction. Earlier short-
acting agents caused serious first-dose hypotension, but the newer
longer-acting agents are far better tolerated.
• These include doxazosin (1–4mg daily).
• Labetalol is an agent that has combined alpha- and beta-blocking
properties, but is not commonly used, except in pregnancy-
induced hypertension.
75.
Renin inhibitors
• Aliskerinis the first orally active renin inhibitor which directly
inhibits plasma renin activity:
• It reduces the negative feedback by which angiotensin II inhibits
renin release. It has been used in combination with ACE inhibitors
and angiotensin receptor blockers with a significant reduction in
blood pressure. Side-effects are few but hypokalaemia occurs.
76.
Other vasodilators
• Theseinclude hydralazine (up to 100 mg daily) and minoxidil (up to
50 mgdaily).
• Both are extremely potent vasodilators that are reserved for patients
resistant to other forms of treatment.
• Hydralazine can be associated with tachycardia, fluid retention and
a systemic lupus erythematosus-like syndrome.
• Minoxidil can cause severe oedema, excessive hair growth and coarse
facial features. If these agents are used, it is usually in combination
with a beta-blocker.
77.
Centrally acting drugs
•Reserpine is used in a low dose of 0.05 mg/day, which provides
almost all its antihypertensive action withfewer side effects than
higher doses. It has a slow onset of action (measured in weeks).
• Methyldopa is still widely used despite central and potentially serious
hepatic and blood side-effects. It acts on central α2-receptors,
usually without slowing the heart.
• Clonidine and moxonidine provide all the benefits of methyldopa with
none of the rare (but serious) autoimmune reactions.
78.
Management of severeor malignant
hypertension
• Patients with severe hypertension (diastolic pressure > 140 mmHg),
malignant hypertension (grades 3 or 4 retinopathy), hypertensive
encephalopathy or with severe hypertensive complications, such as
cardiac failure, should be admitted to hospital for immediate
initiation of treatment.
• However, it is unwise to reduce the blood pressure too rapidly since
this may lead to cerebral, renal, retinal or myocardial infarction, and
the blood pressure response to therapy must be carefully
monitored, preferably in a high dependency unit.
79.
• In mostcases, the aim is to reduce the diastolic blood pressure to
100–110 mmHg over 24–48 hours. This is usually achieved
with oral medication, e.g. atenololor amlodipine. Theblood
pressure can then be normalized over the next 2–3 days.
80.
• When rapidcontrol of blood pressure is required (e.g. in an aortic
dissection), the agent of choice is intravenous sodium
nitroprusside. Alternatively, an infusion of labetalol can be used.
• The infusion dosage must be titrated against the blood pressure
response. Fenoldopam, a selective peripheral dopamine receptor
agonist, is as effective as nitroprusside.
81.
Prognosis
• The prognosisfrom hypertension depends on a number of features:
■ level of blood pressure
■ presence of target-organ changes (retinal, renal, cardiac or
vascular)
■ coexisting risk factors for cardiovascular disease, such as
hyperlipidaemia, diabetes, smoking, obesity, male sex
■ age at presentation.
• Several studies have confirmed that the treatmentof hypertension, even
mild hypertension, will reduce the risk not only of stroke but of
coronary artery disease as well.
#10 GLB.IRB.06.12.01
Reference:
Kearney PM et al. Lancet 2005; 365:217-223
#13 This slide shows the categories of hypertension and the diastolic and systolic pressures associated with them, as defined by: (i) European guidelines (European Society of HypertensionEuropean Society of Cardiology; ESHESC)1 and (ii) US treatment guidelines (Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; JNC 7).2
According to these guidelines, hypertension is defined as a systolic pressure of 140 mmHg or higher and/or a diastolic pressure of 90 mmHg or higher (for an extended time).1,2 The recently updated ESHESC guidelines state, however, that the ‘threshold for hypertension should be considered as flexible based on the level and profile of total cardiovascular risk’.1
In the US guidelines, a category designated ‘pre-hypertension’ is included, and stages 2 and 3 hypertension combined.2 It has recently been reported that patients with pre-hypertension are at increased risk of progression to hypertension.3
References
The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). 2007 guidelines for the management of arterial hypertension. J Hypertens 2007;25:110587.
Chobanian AV, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. JAMA 2003;289:256072.
Schunkert H. Pharmacotherapy for prehypertension mission accomplished?
N Engl J Med 2006;354:17424.












































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




