Download to read offline


![ADHERENCE
‘The extent to which a person's behavior
[in] taking medication following a diet, and
executing lifestyle changes, corresponds
with agreed recommendations from a
health care provider’
- World Health Organization -2003](https://image.slidesharecdn.com/hypertensionadherence-210625154648/85/Hypertension-Non-adherence-to-therapy-11-320.jpg)

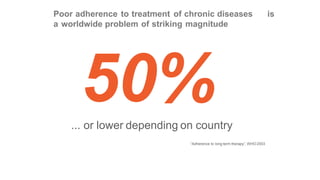


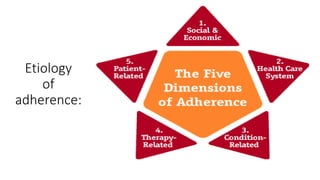





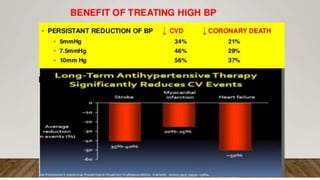
Hypertension is a global health problem affecting over 1 billion people worldwide. Poor adherence to antihypertensive medication regimens is a major challenge for controlling blood pressure. Factors contributing to non-adherence are multi-faceted and include patient-related issues like lack of education on hypertension and its complications, therapy-related challenges like complex dosing protocols and side effects, and health system problems like poor doctor-patient communication. Improving medication adherence requires addressing the underlying causes through patient education, building trust in the doctor-patient relationship, simplifying treatment plans, and utilizing mobile tools and family support.





















































