Downloaded 11 times








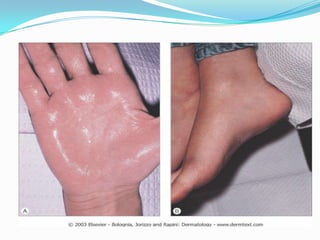







This document discusses hyperhydrosis, or excessive sweating. It defines hyperhydrosis and classifies it as either primary or secondary. Primary hyperhydrosis is associated with overactive sweat glands and often starts in childhood, while secondary is caused by other disorders. Causes mentioned include infections, obesity, and neurological issues. Diagnosis involves examining the patient's history and conducting sweat tests. Treatment options reviewed include topical antiperspirants, oral medications, iontophoresis, botulinum toxin injections, and surgery. The conclusion states that while embarrassing, hyperhydrosis is treatable and need not interfere significantly with one's quality of life.















































