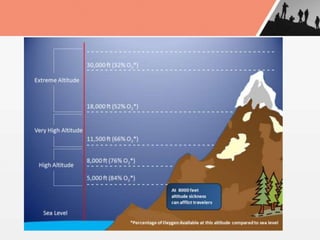
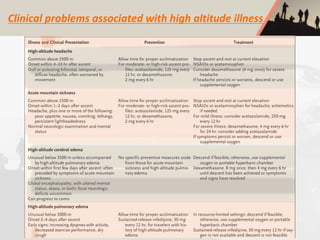
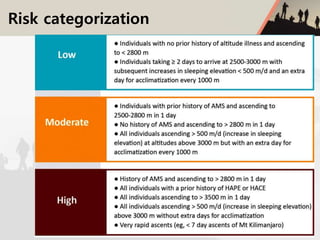
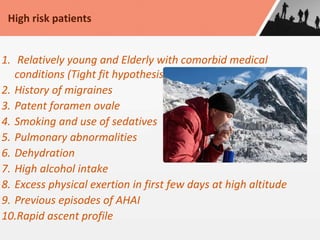
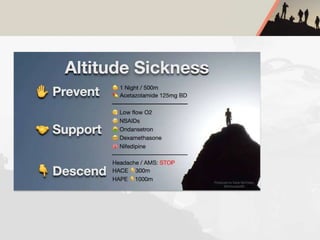
A 25-year-old male presented with shortness of breath and headache 16 hours after ascending to an altitude of 4,200 meters via cable car in Gulmarg, India. On examination, he had a respiratory rate of 36, oxygen saturation of 60% on room air, and clear lung sounds. He was given oxygen, paracetamol, and nifedipine and improved over 4 days, then was discharged. The document discusses various high altitude medical disorders, risk factors, management approaches, and advice for preventing issues like acute mountain sickness.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

