This document discusses hernias, defined as an abnormal protrusion of an organ or tissue through a defect in its surrounding wall. Over 600,000 hernia repairs are performed annually in the US, making it one of the most common operations. Abdominal wall hernias typically occur at sites where the abdominal wall muscles are weak. The majority are inguinal hernias, accounting for around 75% of cases. Hernias can be classified based on site, clinical features, origin, or contents. Increased intra-abdominal pressure and defects or weaknesses in the abdominal wall are the main causes. Surgical repair is the primary treatment, with laparoscopic and open procedures being common options. Post-operative complications

![TYPES/CLASSIFICATION
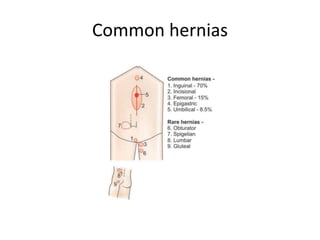
• [1] Based on site
• (a) Inguinal
• (b) Femoral
• (c) Umbilical
• (d) Para-umbilical
• (e) Epigastric
• (f) Spigellian
• (g) Lumbar
linea semilunaris) hernia passes through the Spigelian zone, the
zone of transition between the muscular fibres and aponeurosis
of the transversus abdominis, lateral to the rectus](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-4-320.jpg)
![• [2] Based on Clinical features
• (a) Reducible
• (b) Irreducible
• (c) Complete
• (d) Incomplete
• (e) Obstructed
• (f) Strangulated
• (g) Pantaloon- both direct and indirect sites](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-5-320.jpg)
![• [3] Based on origin
• (a) Congenital
• (b) Acquired including incisional hernias
• [4] Based on content
• (a) Omentocele-omentum
• (b) Enterocele –intestine
• ( c) Cystocele-urinary bladder
• (d) Littre’s hernia-Meckel’s diverticulum](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-6-320.jpg)
![Newer Classification of inguinal
hernias
• [1] Nyhus
• Type I-Indirect hernia with normal deep ring
• Type II-Indirect hernia with dilated deep ring
• Type III- Posterior wall defect
• a-Direct hernia,Sliding hernia
• b-Pantaloon hernia
• c – Femoral
• Type IV-Recurrent herniza](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-8-320.jpg)
![• [2] Gilbert
• [3] Bendavid](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-9-320.jpg)
![AETIOLOGY
• Two main factors
• [1] Defect or weakness in the abdominal wall
• [2] Repeated increased intra-abdominal
pressure
• DEFECT OR WEAKNESS OF THE WALL
• -sites of penetration of a blood vessel
• -Defect may be embryological or anatomical in
origin eg internal inguinal ring,femoral ring,](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-12-320.jpg)
![Relative distribution
• MALES AND FEMALES
• TYPES GHANA USA
• [1] Inguinal 92% 82.5%
• [2] Femoral 2% 4.5%
• [3] Umbil+pa 4% 3.5%
• [4] Incisional 1% 6.5%
• [5] Others 1% 3%](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-16-320.jpg)
![Treatment
• Operative treatment [Herniorrhaphy]
• Open or Laparoscopic
• Anatomic or prosthetic
• Anterior or preperitoneal](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-22-320.jpg)
![Surgeries for inguinal Hernia
• [1] Modified Bassini with Tanner slide
• [2]Shouldice
• [3]Darning
• [4]Tension free repair[Lichtenstein] is the gold
standard](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-23-320.jpg)
![Operations for femoral hernias
• [1]High approach- McEvedy
• [2]Transinguinal approach-Lotheissen
• [3]Low approach -Lockwood](https://image.slidesharecdn.com/hernias-1-220828180116-79e1e22d/85/HERNIAS-1-pptx-24-320.jpg)