This document is a claim form for hospitalization expenses under a health insurance policy with Life Insurance Corporation of India.
The 4-page form requests information about the policyholder, insured member, hospitalization details including dates and hospitals, attending doctors, treatment details, expenses incurred and documents being submitted.
It includes declarations by the policyholder/claimant authorizing access to medical information and confirming inclusion of all relevant documents and bills. The final page is for discharge of the claim and selection of payment method as NEFT/RTGS or demand draft along with bank account details.
Proposal form is the most important and basic document required for life insurance contract between the insured and insurance company. It includes the insured's basic information like address, age, name, education, occupation etc. It also includes the person's medical history.
Health plus claim is a part of life insurance. Issuance of this form does not amount to admission of any liability under the claim on the part of the insurers.
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Proposal form is the most important and basic document required for life insurance contract between the insured and insurance company. It includes the insured's basic information like address, age, name, education, occupation etc. It also includes the person's medical history.
Health plus claim is a part of life insurance. Issuance of this form does not amount to admission of any liability under the claim on the part of the insurers.
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
ESIC Benefits | Only for the Private Use for the Staff of SandMartin Group of Companies & should not be treated as professional opinion/recommendations.
FAQs on CGHS are intended to provide general information and guidance needed for the CGHS beneficiaries to avail CGHS facilities The contents must be read in conjunction with OMs/Office orders as issued from time to time.
This ppt is the summery of ESIC topic, i have tried to explain the procedures involved in ESI with my FAQ segments.
Hoping you all will like and appreciate it...
A sample form of application for Indian Passport uploaded by T. J Joseph Adhikarathil,Deputy Tahsildar, Kottayam,Mob 9447464502. A mysandesham presentation.Form of application for passport,Government of India.
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Health plus claim intimation form is for Health Insurance Policies (HCB & MSB Claims).Form must be completed & signed by Policy Holder / Principal Insured only and submitted to the TPA.
ESIC Benefits | Only for the Private Use for the Staff of SandMartin Group of Companies & should not be treated as professional opinion/recommendations.
FAQs on CGHS are intended to provide general information and guidance needed for the CGHS beneficiaries to avail CGHS facilities The contents must be read in conjunction with OMs/Office orders as issued from time to time.
This ppt is the summery of ESIC topic, i have tried to explain the procedures involved in ESI with my FAQ segments.
Hoping you all will like and appreciate it...
A sample form of application for Indian Passport uploaded by T. J Joseph Adhikarathil,Deputy Tahsildar, Kottayam,Mob 9447464502. A mysandesham presentation.Form of application for passport,Government of India.
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Health plus claim intimation form is for Health Insurance Policies (HCB & MSB Claims).Form must be completed & signed by Policy Holder / Principal Insured only and submitted to the TPA.
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Hospital treatment form is also a part of health insurance policies.These forms are also useful in case of medical insurance and to be filled in by the Hospital.If the treatment is from more than one hospital, forms from all the hospitals must be filled and submitted.
Pre- Authorization form is to be filled in case of hospitalization. It is basically a declaration by the patient to make claim for the expenses incurred during the hospitalization. While seeking health insurance coverage under Optima Restore, the Pre- Authorization form must be filled to avail the policy support. Through this Apollo Munich seek information about the patient or the insured person like name of the patient, contact details, age, policy number and card ID number, name of the hospital, nature of illness and other related details. All columns must be closely examined to provide genuine information to the insurer. The form must be duly filled and then must be attached with all the necessary documents absence of which can lead to complication.
Pre- Authorization form is to be filled in case of hospitalization. It is basically a declaration by the patient to make claim for the expenses incurred during the hospitalization. Easy Health Pre- Authorization form will seek information about the patient or the insured person like name of the patient, contact details, age, policy number and card ID number, name of the hospital, nature of illness and other related details. All columns must be closely examined to provide genuine information to the insurer. The form must be duly filled and then must be attached with all the necessary documents to avail the service.
Apollo Munich claim procedure is easy to understand with information provided in simple and uncomplicated wordings. Insure Health claim form is easily available on the website of the company. The form is to filled while filing the claim for insured illness.
The form seeks basic information like policy number, contact details, name of the insured and details regarding the illness for which the claim is to be filed. However, the insured need to be sure of the information provided. Details provided must be correct and complete to receive the listed benefits. In case of any dishonest information provided, the benefits will be forfeited making the policy void. With a ready link to Claim Form on the website, all customers can move ahead with the procedure.
Pre- Authorization form is to be filled in case of hospitalization. It is basically a declaration by the patient to make claim for the expenses incurred during the hospitalization. While seeking health insurance coverage under Optima Plus, the Pre- Authorization form must be filled to avail the policy support. Through this Apollo Munich seek information about the patient or the insured person like name of the patient, contact details, age, policy number and card ID number, name of the hospital, nature of illness and other related details. All columns must be closely examined to provide genuine information to the insurer. The form must be duly filled and attached with all the necessary documents absence of which can lead to complication.
Notice of change of nomination form 3750sm123services
With a vision of becoming Delhi’s most admired INSURANCE Company, SM Services offers you to Buy Insurance Online. Insurance is a contract (insurance coverage) where the insurance provider (insurance policy company) concurs for a cost (insurance coverage premiums) to pay the insured event all or a part of any loss endured by accident or death.
With a vision of becoming Delhi’s most admired INSURANCE Company, SM Services offers you to Buy Insurance Online. Insurance is a contract (insurance coverage) where the insurance provider (insurance policy company) concurs for a cost (insurance coverage premiums) to pay the insured event all or a part of any loss endured by accident or death.
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Life insurance is a contract between you and the life insurance company (the insurer), which provides you (the assured) or your beneficiary for whose benefit the policy is taken with a pre-determined amount on the happening of a particular event contingent on the duration of human life
Maturity claim form is to be filled by the person legally entitled for the policy maturity benefits.This claim form is for maturity value of endowment assurance/anticipated endowment assurance /yugal suraksha/children policy.
Navy personal questionare is a part of life insurance. This form is for the branch of the naval forces, etc. It includes general information about their present rank, their duties, etc.
Skye Residences | Extended Stay Residences Near Toronto Airportmarketingjdass
Experience unparalleled EXTENDED STAY and comfort at Skye Residences located just minutes from Toronto Airport. Discover sophisticated accommodations tailored for discerning travelers.
Website Link :
https://skyeresidences.com/
https://skyeresidences.com/about-us/
https://skyeresidences.com/gallery/
https://skyeresidences.com/rooms/
https://skyeresidences.com/near-by-attractions/
https://skyeresidences.com/commute/
https://skyeresidences.com/contact/
https://skyeresidences.com/queen-suite-with-sofa-bed/
https://skyeresidences.com/queen-suite-with-sofa-bed-and-balcony/
https://skyeresidences.com/queen-suite-with-sofa-bed-accessible/
https://skyeresidences.com/2-bedroom-deluxe-queen-suite-with-sofa-bed/
https://skyeresidences.com/2-bedroom-deluxe-king-queen-suite-with-sofa-bed/
https://skyeresidences.com/2-bedroom-deluxe-queen-suite-with-sofa-bed-accessible/
#Skye Residences Etobicoke, #Skye Residences Near Toronto Airport, #Skye Residences Toronto, #Skye Hotel Toronto, #Skye Hotel Near Toronto Airport, #Hotel Near Toronto Airport, #Near Toronto Airport Accommodation, #Suites Near Toronto Airport, #Etobicoke Suites Near Airport, #Hotel Near Toronto Pearson International Airport, #Toronto Airport Suite Rentals, #Pearson Airport Hotel Suites
LA HUG - Video Testimonials with Chynna Morgan - June 2024Lital Barkan
Have you ever heard that user-generated content or video testimonials can take your brand to the next level? We will explore how you can effectively use video testimonials to leverage and boost your sales, content strategy, and increase your CRM data.🤯
We will dig deeper into:
1. How to capture video testimonials that convert from your audience 🎥
2. How to leverage your testimonials to boost your sales 💲
3. How you can capture more CRM data to understand your audience better through video testimonials. 📊
What are the main advantages of using HR recruiter services.pdfHumanResourceDimensi1
HR recruiter services offer top talents to companies according to their specific needs. They handle all recruitment tasks from job posting to onboarding and help companies concentrate on their business growth. With their expertise and years of experience, they streamline the hiring process and save time and resources for the company.
VAT Registration Outlined In UAE: Benefits and Requirementsuae taxgpt
Vat Registration is a legal obligation for businesses meeting the threshold requirement, helping companies avoid fines and ramifications. Contact now!
https://viralsocialtrends.com/vat-registration-outlined-in-uae/
Personal Brand Statement:
As an Army veteran dedicated to lifelong learning, I bring a disciplined, strategic mindset to my pursuits. I am constantly expanding my knowledge to innovate and lead effectively. My journey is driven by a commitment to excellence, and to make a meaningful impact in the world.
Memorandum Of Association Constitution of Company.pptseri bangash
www.seribangash.com
A Memorandum of Association (MOA) is a legal document that outlines the fundamental principles and objectives upon which a company operates. It serves as the company's charter or constitution and defines the scope of its activities. Here's a detailed note on the MOA:
Contents of Memorandum of Association:
Name Clause: This clause states the name of the company, which should end with words like "Limited" or "Ltd." for a public limited company and "Private Limited" or "Pvt. Ltd." for a private limited company.
https://seribangash.com/article-of-association-is-legal-doc-of-company/
Registered Office Clause: It specifies the location where the company's registered office is situated. This office is where all official communications and notices are sent.
Objective Clause: This clause delineates the main objectives for which the company is formed. It's important to define these objectives clearly, as the company cannot undertake activities beyond those mentioned in this clause.
www.seribangash.com
Liability Clause: It outlines the extent of liability of the company's members. In the case of companies limited by shares, the liability of members is limited to the amount unpaid on their shares. For companies limited by guarantee, members' liability is limited to the amount they undertake to contribute if the company is wound up.
https://seribangash.com/promotors-is-person-conceived-formation-company/
Capital Clause: This clause specifies the authorized capital of the company, i.e., the maximum amount of share capital the company is authorized to issue. It also mentions the division of this capital into shares and their respective nominal value.
Association Clause: It simply states that the subscribers wish to form a company and agree to become members of it, in accordance with the terms of the MOA.
Importance of Memorandum of Association:
Legal Requirement: The MOA is a legal requirement for the formation of a company. It must be filed with the Registrar of Companies during the incorporation process.
Constitutional Document: It serves as the company's constitutional document, defining its scope, powers, and limitations.
Protection of Members: It protects the interests of the company's members by clearly defining the objectives and limiting their liability.
External Communication: It provides clarity to external parties, such as investors, creditors, and regulatory authorities, regarding the company's objectives and powers.
https://seribangash.com/difference-public-and-private-company-law/
Binding Authority: The company and its members are bound by the provisions of the MOA. Any action taken beyond its scope may be considered ultra vires (beyond the powers) of the company and therefore void.
Amendment of MOA:
While the MOA lays down the company's fundamental principles, it is not entirely immutable. It can be amended, but only under specific circumstances and in compliance with legal procedures. Amendments typically require shareholder
Business Valuation Principles for EntrepreneursBen Wann
This insightful presentation is designed to equip entrepreneurs with the essential knowledge and tools needed to accurately value their businesses. Understanding business valuation is crucial for making informed decisions, whether you're seeking investment, planning to sell, or simply want to gauge your company's worth.
Attending a job Interview for B1 and B2 Englsih learnersErika906060
It is a sample of an interview for a business english class for pre-intermediate and intermediate english students with emphasis on the speking ability.
Falcon stands out as a top-tier P2P Invoice Discounting platform in India, bridging esteemed blue-chip companies and eager investors. Our goal is to transform the investment landscape in India by establishing a comprehensive destination for borrowers and investors with diverse profiles and needs, all while minimizing risk. What sets Falcon apart is the elimination of intermediaries such as commercial banks and depository institutions, allowing investors to enjoy higher yields.
RMD24 | Retail media: hoe zet je dit in als je geen AH of Unilever bent? Heid...BBPMedia1
Grote partijen zijn al een tijdje onderweg met retail media. Ondertussen worden in dit domein ook de kansen zichtbaar voor andere spelers in de markt. Maar met die kansen ontstaan ook vragen: Zelf retail media worden of erop adverteren? In welke fase van de funnel past het en hoe integreer je het in een mediaplan? Wat is nu precies het verschil met marketplaces en Programmatic ads? In dit half uur beslechten we de dilemma's en krijg je antwoorden op wanneer het voor jou tijd is om de volgende stap te zetten.
Premium MEAN Stack Development Solutions for Modern BusinessesSynapseIndia
Stay ahead of the curve with our premium MEAN Stack Development Solutions. Our expert developers utilize MongoDB, Express.js, AngularJS, and Node.js to create modern and responsive web applications. Trust us for cutting-edge solutions that drive your business growth and success.
Know more: https://www.synapseindia.com/technology/mean-stack-development-company.html
Buy Verified PayPal Account | Buy Google 5 Star Reviewsusawebmarket
Buy Verified PayPal Account
Looking to buy verified PayPal accounts? Discover 7 expert tips for safely purchasing a verified PayPal account in 2024. Ensure security and reliability for your transactions.
PayPal Services Features-
🟢 Email Access
🟢 Bank Added
🟢 Card Verified
🟢 Full SSN Provided
🟢 Phone Number Access
🟢 Driving License Copy
🟢 Fasted Delivery
Client Satisfaction is Our First priority. Our services is very appropriate to buy. We assume that the first-rate way to purchase our offerings is to order on the website. If you have any worry in our cooperation usually You can order us on Skype or Telegram.
24/7 Hours Reply/Please Contact
usawebmarketEmail: support@usawebmarket.com
Skype: usawebmarket
Telegram: @usawebmarket
WhatsApp: +1(218) 203-5951
USA WEB MARKET is the Best Verified PayPal, Payoneer, Cash App, Skrill, Neteller, Stripe Account and SEO, SMM Service provider.100%Satisfection granted.100% replacement Granted.
Putting the SPARK into Virtual Training.pptxCynthia Clay
This 60-minute webinar, sponsored by Adobe, was delivered for the Training Mag Network. It explored the five elements of SPARK: Storytelling, Purpose, Action, Relationships, and Kudos. Knowing how to tell a well-structured story is key to building long-term memory. Stating a clear purpose that doesn't take away from the discovery learning process is critical. Ensuring that people move from theory to practical application is imperative. Creating strong social learning is the key to commitment and engagement. Validating and affirming participants' comments is the way to create a positive learning environment.
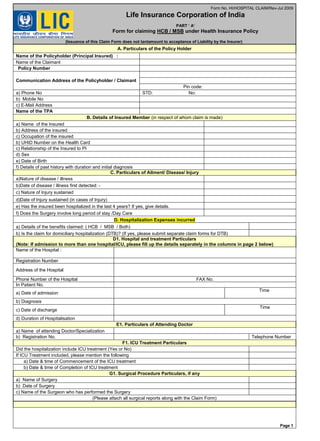
1. Form No. HI/HOSPITAL CLAIM/Rev-Jul 2009
Life Insurance Corporation of India
PART ‘ A’
Form for claiming HCB / MSB under Health Insurance Policy
(Issuance of this Claim Form does not tantamount to acceptance of Liability by the Insurer)
A. Particulars of the Policy Holder
Name of the Policyholder (Principal Insured) :
Name of the Claimant
Policy Number
Communication Address of the Policyholder / Claimant
Pin code:
a) Phone No STD: No:
b) Mobile No
c) E-Mail Address
Name of the TPA
B. Details of Insured Member (in respect of whom claim is made)
a) Name of the Insured
b) Address of the insured
c) Occupation of the insured
b) UHID Number on the Health Card
c) Relationship of the Insured to PI
d) Sex
e) Date of Birth
f) Details of past history with duration and initial diagnosis
C. Particulars of Ailment/ Disease/ Injury
a)Nature of disease / illness
b)Date of disease / illness first detected: -
c) Nature of Injury sustained
d)Date of Injury sustained (in cases of Injury)
e) Has the insured been hospitalized in the last 4 years? If yes, give details.
f) Does the Surgery involve long period of stay /Day Care
D. Hospitalization Expenses incurred
a) Details of the benefits claimed: ( HCB / MSB / Both)
b) Is the claim for domiciliary hospitalization (DTB)? (If yes, please submit separate claim forms for DTB)
D1. Hospital and treatment Particulars
(Note: If admission to more than one hospital/ICU, please fill up the details separately in the columns in page 2 below)
Name of the Hospital :
Registration Number
Address of the Hospital
Phone Number of the Hospital FAX No.
In Patient No.
a) Date of admission
Time
b) Diagnosis
c) Date of discharge
Time
d) Duration of Hospitalisation
E1. Particulars of Attending Doctor
a) Name of attending Doctor/Specialization
b) Registration No. Telephone Number
F1. ICU Treatment Particulars
Did the hospitalization include ICU treatment (Yes or No)
If ICU Treatment included, please mention the following
a) Date & time of Commencement of the ICU treatment
b) Date & time of Completion of ICU treatment
G1. Surgical Procedure Particulars, if any
a) Name of Surgery
b) Date of Surgery
c) Name of the Surgeon who has performed the Surgery
(Please attach all surgical reports along with the Claim Form)
Page 1
2. D2. Hospital and treatment Particulars
(Note: If admission to more than one hospital/ICU, please fill up the details separately in the columns below)
Name of the Hospital :
Registration Number
Address of the Hospital
Phone Number of the Hospital
FAX Number of the Hospital
a) Date of admission Time
b) Diagnosis
c) Date of discharge Time
d) Duration of Hospitalisation
E2. Particulars of Attending Doctor
a) Name of attending Doctor
b) Registration No. Telephone Number
F2. ICU Treatment Particulars
Did the hospitalization include ICU treatment (Yes
or No)
If ICU Treatment included, please mention the
following
a) Date of Commencement of the ICU treatment Time:
b) Date of Completion of ICU treatment Time:
G2. Surgical Procedure Particulars, if any
a) Name of Surgery
b) Date of Surgery
c) Name of the Surgeon who has performed the
Surgery
(Please attach all surgical reports along with the Claim Form)
D3. Hospital and treatment Particulars
(Note: If admission to more than one hospital/ICU, please fill up the details separately in the columns below)
Name of the Hospital :
Registration Number
Address of the Hospital
Phone Number of the Hospital
FAX Number of the Hospital
a) Date of admission Time
b) Diagnosis
c) Date of discharge Time
d) Duration of Hospitalisation
E3. Particulars of Attending Doctor
a) Name of attending Doctor
b) Registration No. Telephone Number
F3. ICU Treatment Particulars
Did the hospitalization include ICU treatment (Yes or No)
If ICU Treatment included, please mention the following
a) Date & time of Commencement of the ICU treatment
b) Date & time of Completion of ICU treatment
G3. Surgical Procedure Particulars, if any
a) Name of Surgery
b) Date of Surgery
c) Name of the Surgeon who has performed the Surgery
(Please attach all surgical reports along with the Claim Form)
H. Details of the Other Healthl Insurance Claims made by the Policy Holder / Claimant
Is there a simultaneous claim being made on any Health Insurance policy other than Health Plus plan of LIC of India held by the Insured
Member? Is so, please give details of the policy such as – Date of commencement, amount, covered members.
_______________________________________________________________________________________
Policy Number Dt of commencement Servicing Division HCB covered Remarks
Declaration by the Policy Holder / Claimant
I hereby declare that the above information is true & correct to the best of my knowledge and belief. If I have made any false, fraud or
untrue statement, suppression or concealment, my right to claim under the policy shall be forfeited.
Date:
Place: Signature of the Policyholder/Claimant
Page2
3. Schedule of Expenses incurred
Date Bill No.
Description
(Mention type of
Bill)
Bill issued by
Amount
Claimed.
Mention type
of expenses
Hospitalization Remarks
Total
I have incurred the expenses shown above for the treatment of the disease / illness / accident.
In support of the claim, I enclose the following documents
YES --NO YES --NO
Policy Schedule / Policy Copy Claim Form attested by the Hospital (See Page 3)
Hospital Bills / Records etc
Hospital Final Bill* 1. Hospital Payment Receipt/s
Discharge Summary / Discharge card* 2. MRI report/receipt
Doctors Surgery Certificate if any 3. CT Scan report/receipt
Surgery / Consultation Bills if any 4. ECG report/receipt
Medicine bills with Doctors prescription 5. X-ray report/receipt
Investigation Reports with Doctors advice 6. US Scan report/receipt
Lab Reports with Doctors request No(s). of Reports 7. Others (Specify)
Death Certificate (if applicable)
MLC copy (if applicable)
(Copies of the bills duly attested by Hospital Authorities would suffice -Bills once submitted will NOT be returned)
* (If more than one hospital, please attach the copies of the Discharge/Discharge Card of all the hospitals)
Page 3
Declaration
I hereby authorize the representatives of the TPA, M/s_________________________________ and Life Insurance Corporation of
India free and unlimited access to seek medical information (Indoor case papers, reports, documents, including photocopies
thereof/pertaining my admission/treatment etc.,) from any hospital/medical practitioner from which or whom I have/the Insured
member has at any time sought or shall seek medical attention concerning any disease/sickness, ailment or injury, which affects my
physical or mental health.
I hereby declare that I have included all bills/ receipts for the purpose of this claim and I will not be making any supplementary claim
in this regard.
I also hereby authorize the hospital/attending doctor/medical practitioner from whom I have/the Insured member has sought
medical attention/medical treatment concerning any disease/sickness, ailment or injury which affected my/insured members
physical/mental health to part with the above information to the TPA/LIC of India or its representatives. Myself/my
successors/assigns shall not raise any dispute or litigation on passing of such information to the TPA or LIC of India or its
representatives.
Date & Place
Signature of the Policy Holder /Claimant
Please Note to submit this "Claim Form" with all the enclosures to your TPA only
(Issuance of this Claim Form does not tantamount to acceptance of Liability by the Insurer)
___________________________________________________________
4. Claim Discharge Form
Policy No :___________________________
Name of the Principal Insured:___________________________
I hereby authorize Life Insurance Corporation of India to make payment of the above
claim, admissible as per terms, conditions and limitations of the Policy. This
discharge is delivered in full and final settlement of the hospital bills submitted by
me and to the full satisfaction of my above mentioned claim.
1
Option to be provided by the
Policyholder for Claim payment
to be made by NEFT/RTGS or
Demand Draft
ELECTRONIC MODE OF TRANFER
(For NEFT/RTGS transfer – please furnish your bank
account details in question 2 below)
Demand Draft
2
DETAILS OF THE BANK A/C TO
WHICH THE POLICYHOLDER
DESIRES TRANSFER OF CLAIM
AMOUNT
NAME OF THE BANK ------------------------------
-----------------------------------------------------
Location -------------------------------------------
Branch Code --------------------------------------
*
A/C NO--------------------------------------------
IFSC NO-------------------------------------------
(The eleven digit number that will enable payments
through RTGS/NEFT – credited into your account)
( * Please attach a cancelled cheque leaf to authenticate the details given)
The details of Bank account and address of the bank etc furnished by me above are
correct and I hereby authorize Life Insurance Corporation of India to make the claim
payment to my above mentioned Bank Account
DATED AT--------------------------------------THIS --------------------DAY OF------------------------200
Place: SIGNATURE OF THE POLICYHOLDER/ CLAIMANT
Name : ______________________________.
Address: _____________________________________.
______________________________________.
(Issuance of this Claim Form does not tantamount to acceptance of Liability by the Insurer)
Page 4
Revenue
Stamp