Download to read offline
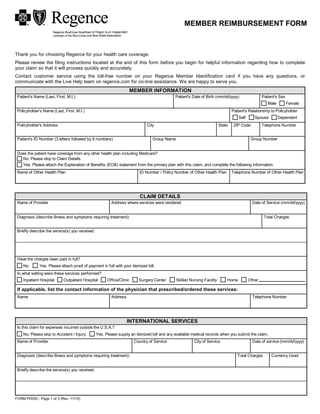



This document is a reimbursement form for ABCDE health plan members. It requests information about the patient and claim, including patient details, other insurance coverage, service provider information, and a description of the medical issue and treatment. Members are instructed to attach an itemized bill and any other necessary documentation, sign the form, and mail it to the claims address provided for processing.