Download as PDF, PPTX













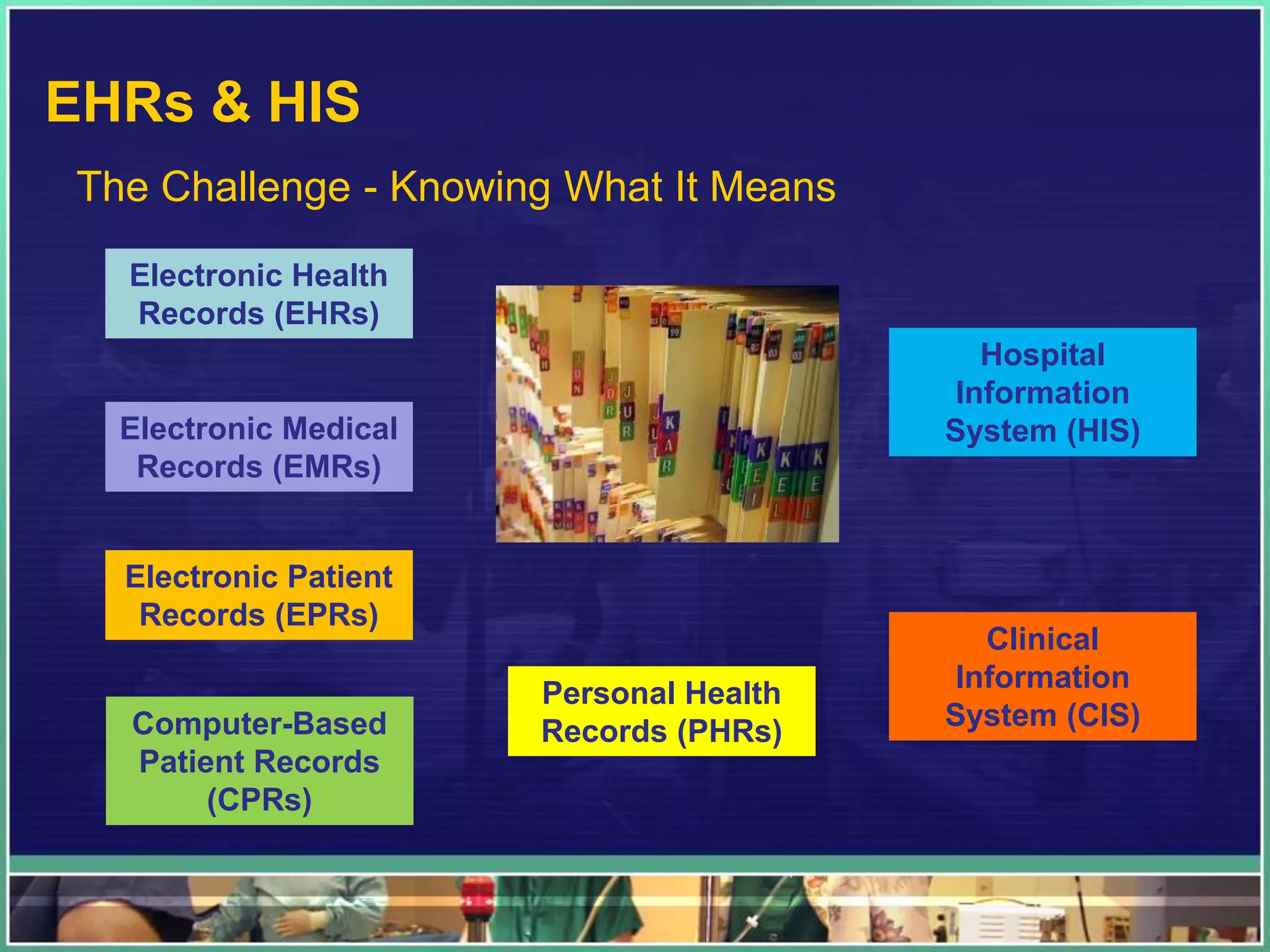
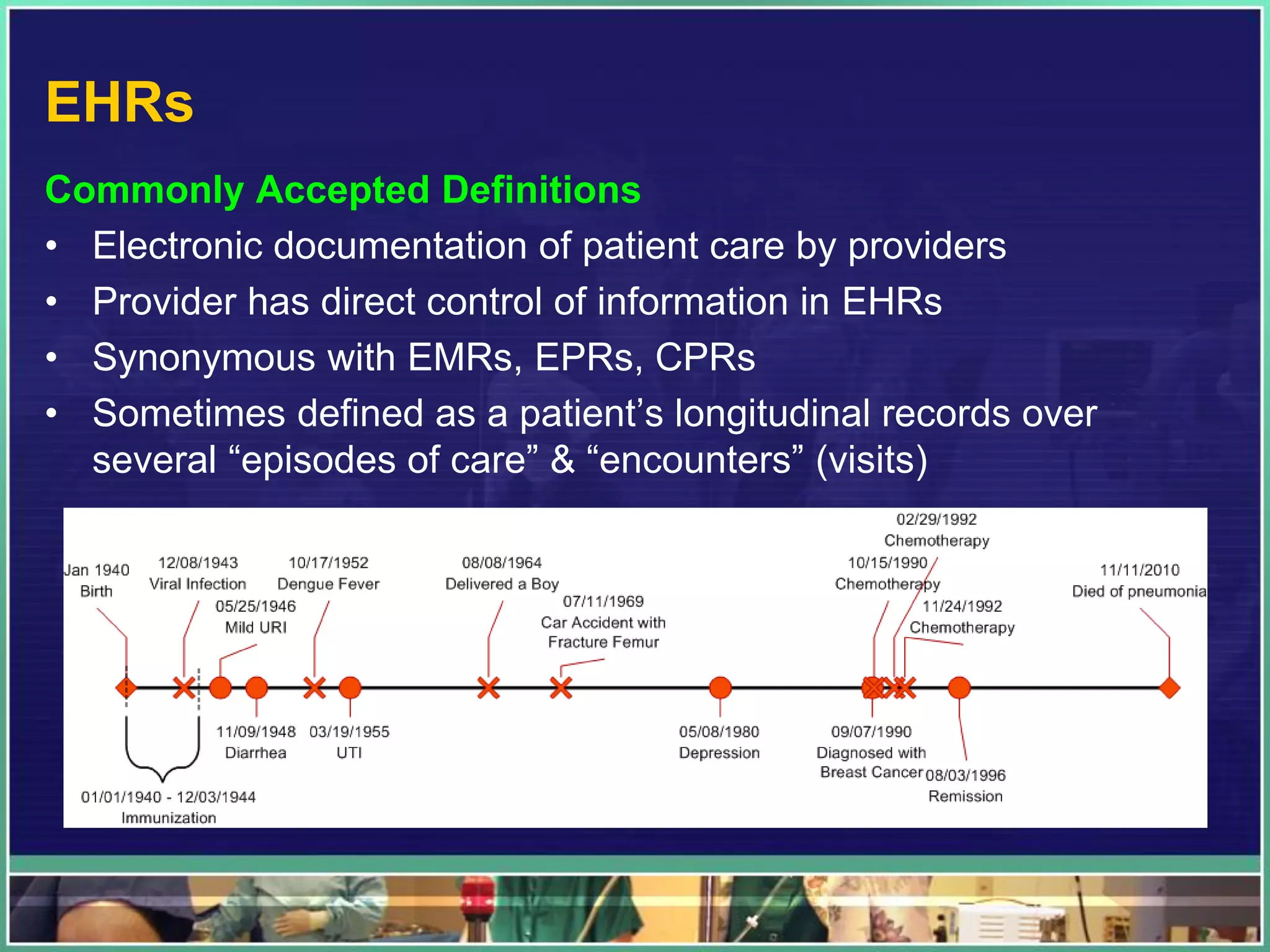






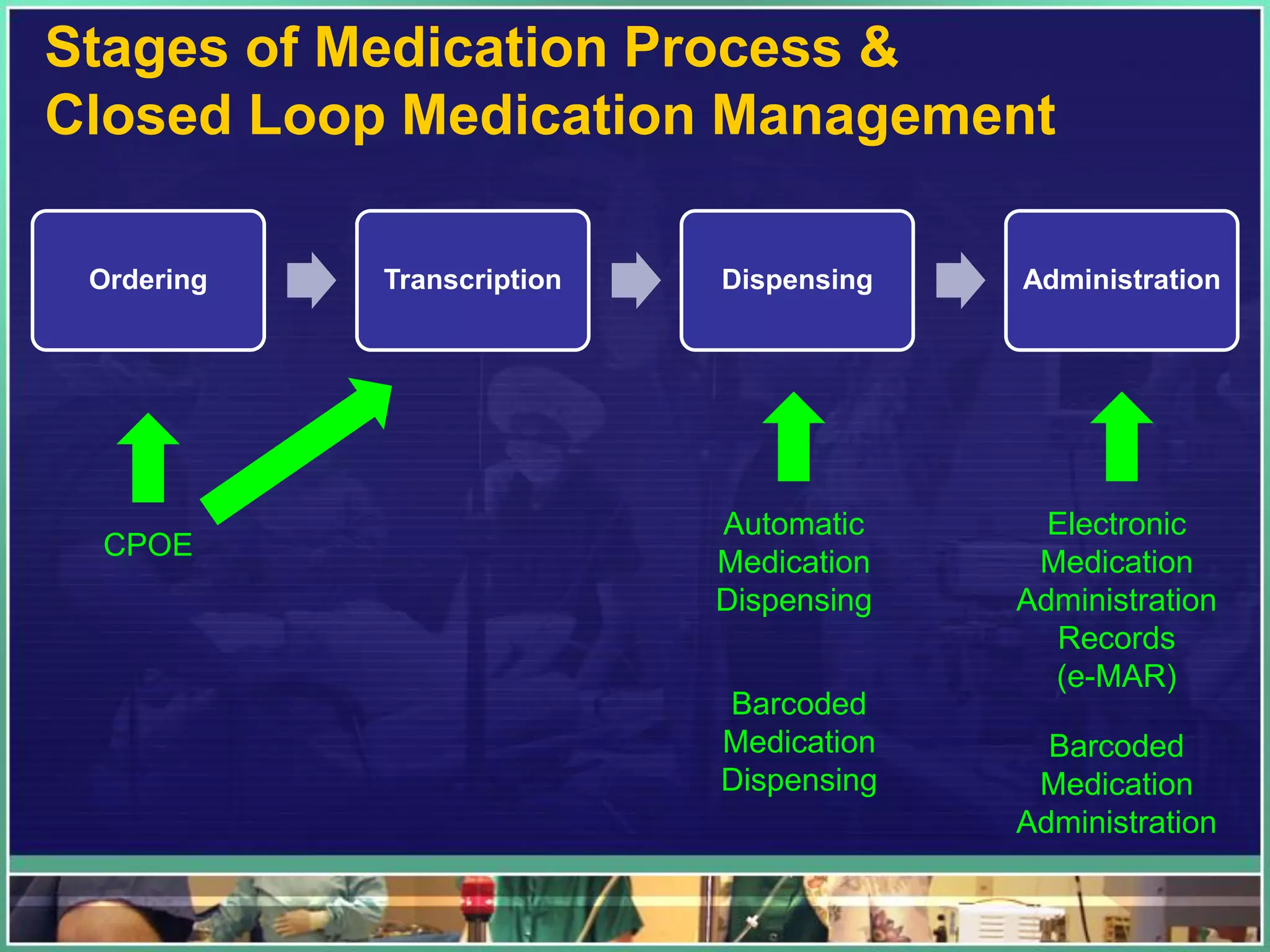
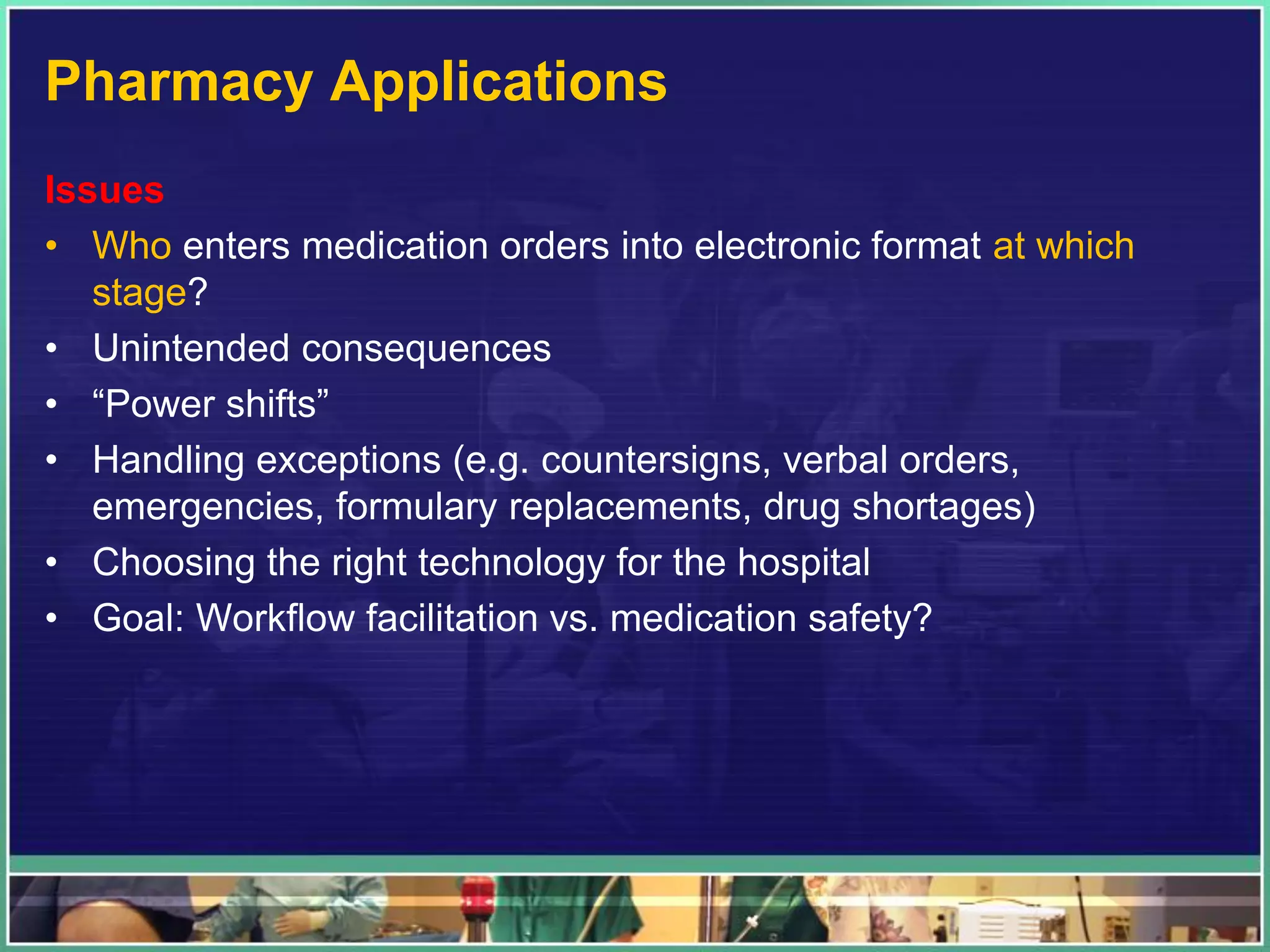






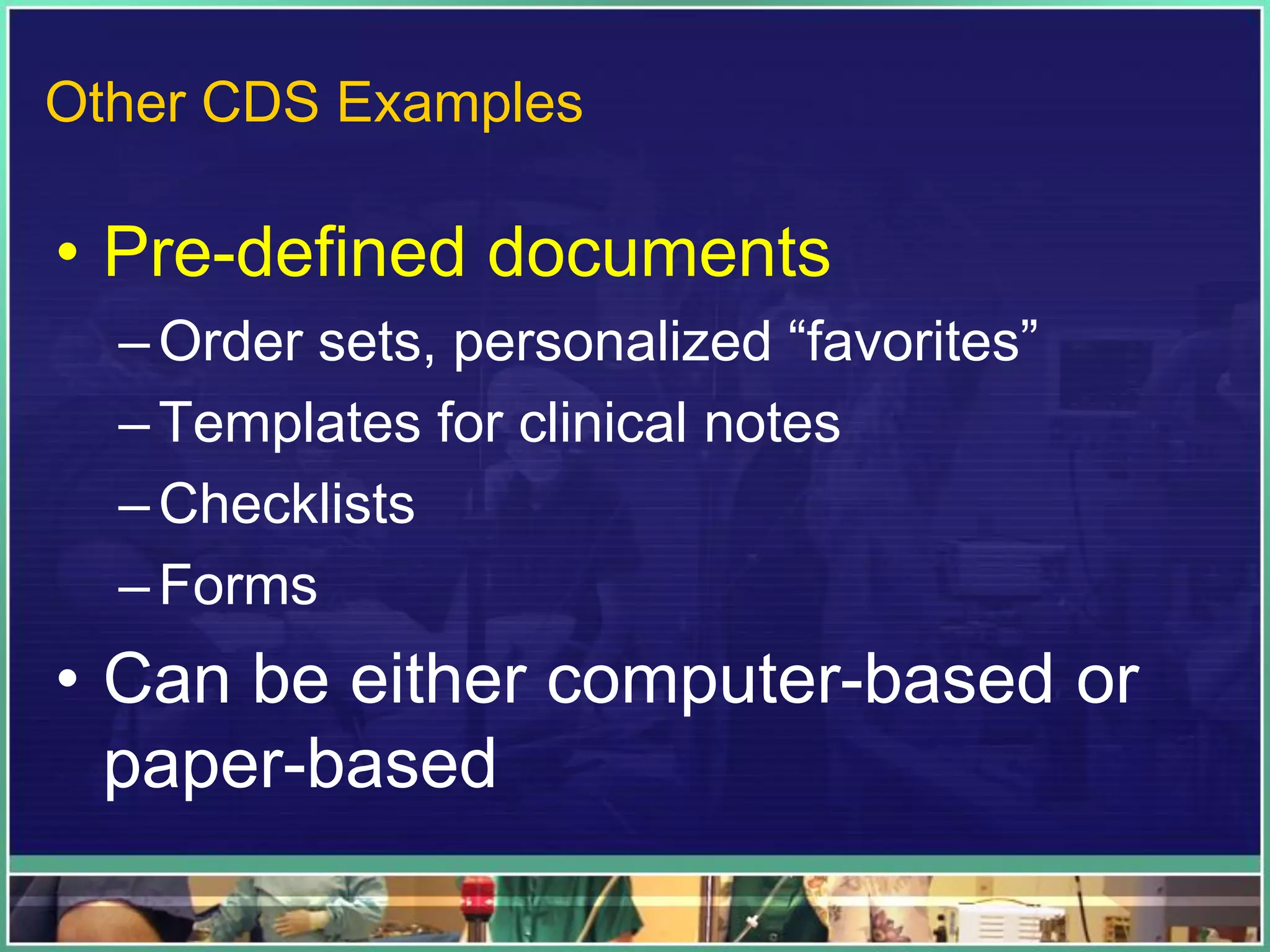
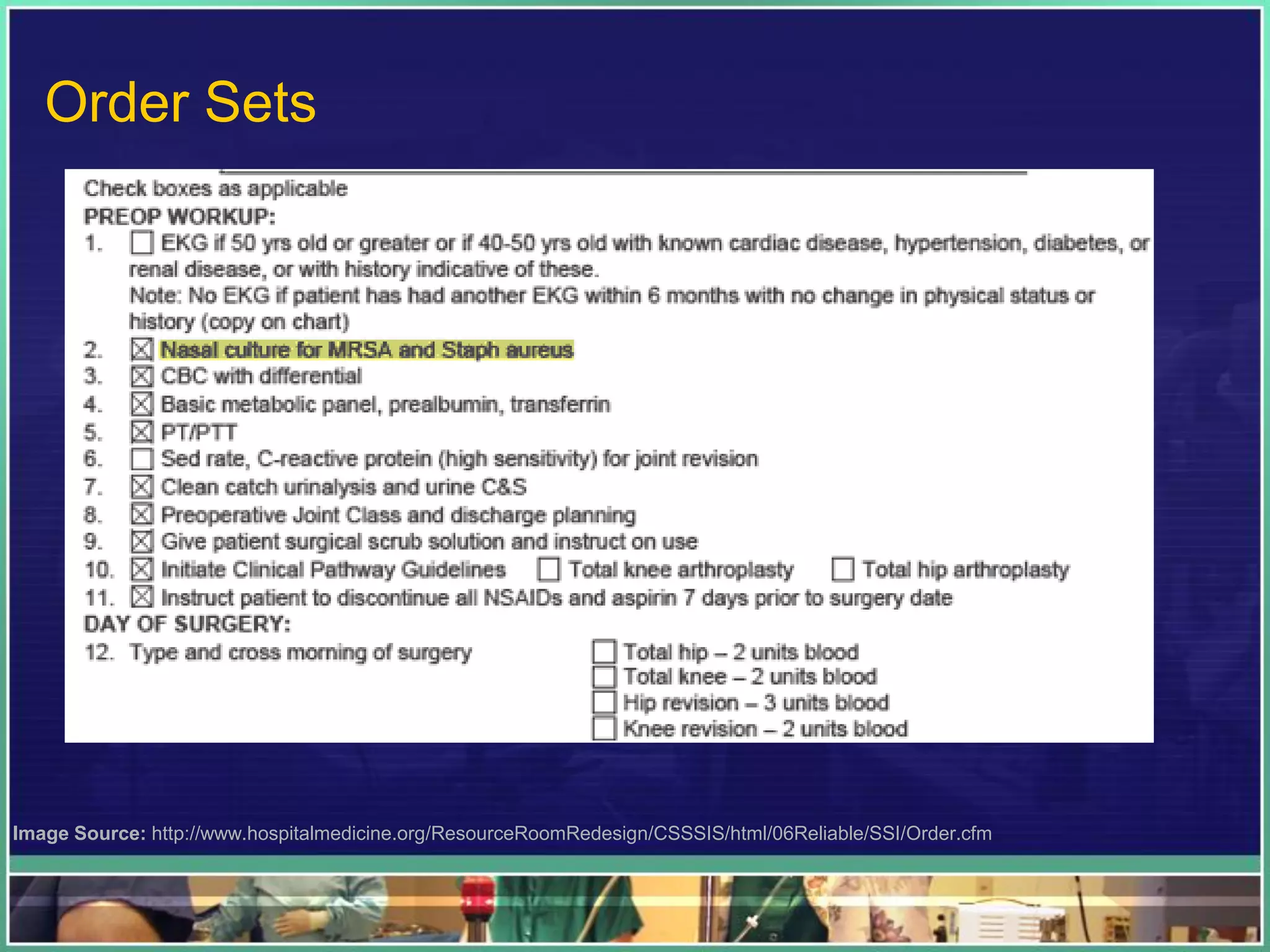














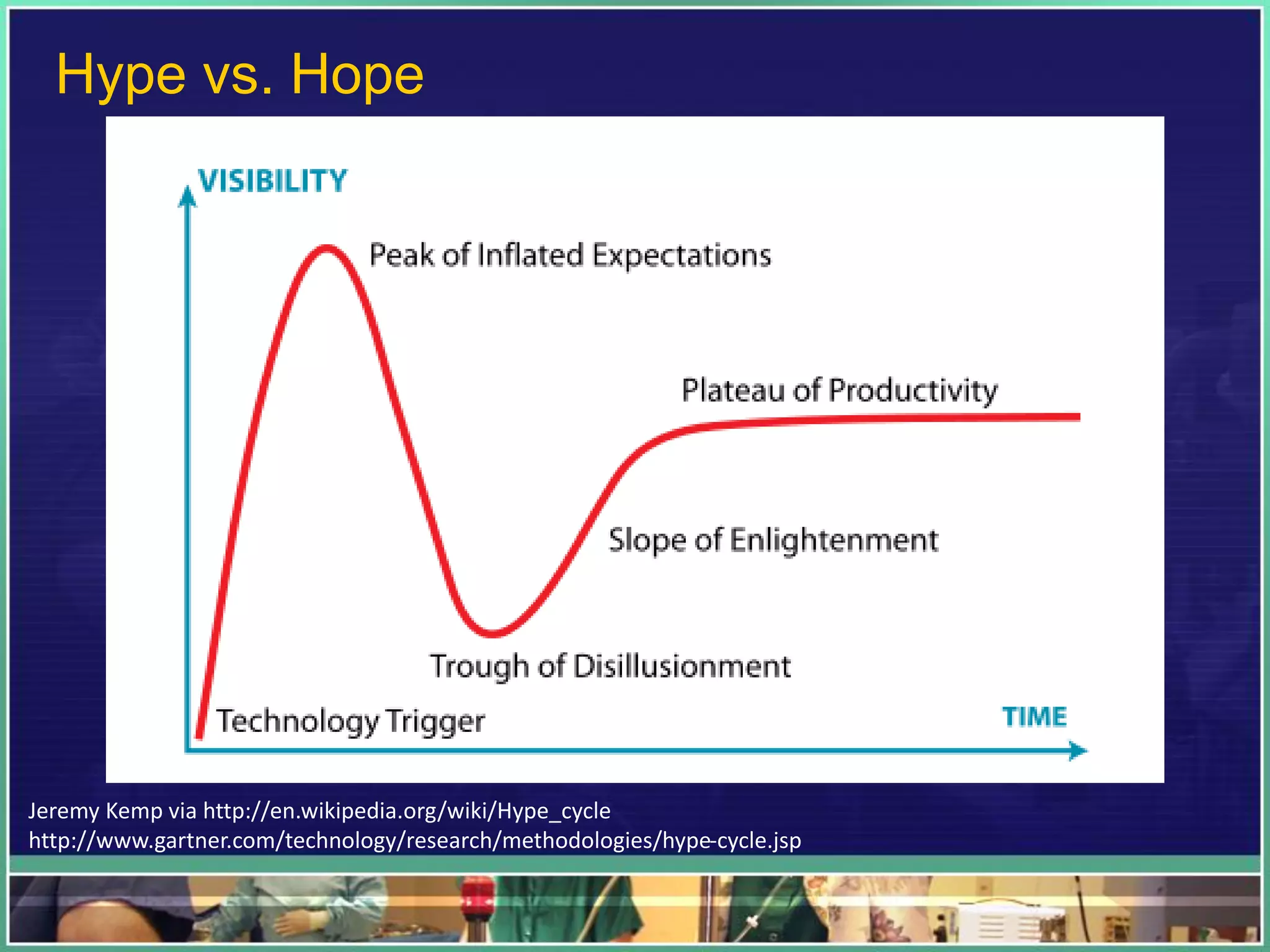



















This document discusses health IT in clinical settings and provides 3 key points: 1. IT implementation success depends on factors like business-IT alignment, understanding the local organizational context, and focusing on real goals rather than IT as the end goal. 2. Examples of important hospital IT systems include EHRs, CPOE, clinical decision support systems, imaging applications like PACS, and pharmacy applications. Key issues involve usability, integration, and change management. 3. While health IT and "smart" machines offer benefits, clinical judgment is still necessary given variability in patients and medicine. The goal is high quality, patient-centered care; technology should improve information and processes, not replace humans. Unint























































































