Downloaded 76 times


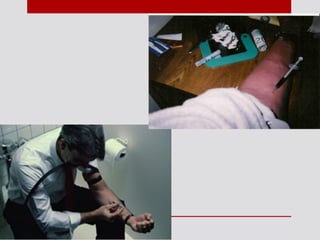
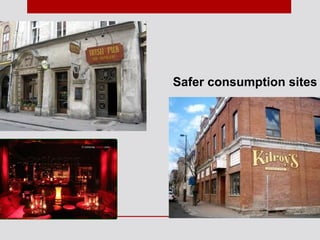


This document discusses harm reduction, its goals and strategies. It defines harm reduction as policies and programs that aim to reduce health and social harms of drug use without requiring decreased use. The goals of harm reduction include empowering users to make safer choices and reducing transmission of diseases. Common strategies mentioned include needle exchange programs and supervised injection sites. The document also explores myths around harm reduction and its application among special populations such as Indigenous communities.