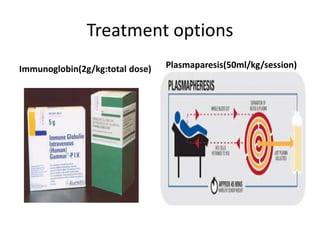
This document discusses Gullain-Barre syndrome (GBS), including that it is the leading cause of acute flaccid paralysis in developed countries. GBS causes muscle weakness that starts in the legs and progresses upwards in an acute and symmetric manner. Ventilation is required in 25% of cases and 4-15% of patients die from GBS. The document outlines clinical features, variants of GBS, diagnostic tests including lumbar puncture and nerve conduction studies, treatment including immunoglobulin or plasmapheresis, and criteria for diagnosing GBS.